



Abstract
Background
The benefits and adverse effects of corticosteroids in the treatment of severe community-acquired
pneumonia (CAP) have not been well assessed. The aim of this systematic review of
the literature and meta-analysis was to evaluate the clinical efficacy of adjuvant
corticosteroid therapy in patients with severe CAP.
Methods
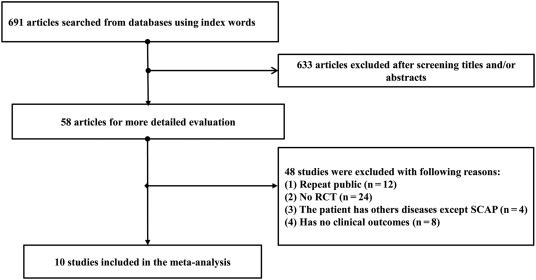
The following databases were searched: PubMed, the Cochrane database, Embase, Wanfang,
the China National Knowledge Infrastructure (CNKI), and the WeiPu (VIP) database in
Chinese. Published randomized controlled clinical trial results were identified that
compared corticosteroid therapy with conventional therapy for patients with severe
CAP, up to November 2016. The relative risk (RR), weighted mean difference (WMD),
and 95% confidence interval (CI) were evaluated. Statistical analysis was performed
using STATA 10.0. The quality of the published studies was evaluated using the Oxford
quality scoring system (Jadad scale).
Results
Ten randomized controlled trials (RCTs) were identified that included 729 patients
with severe CAP. Data analysis showed that corticosteroid therapy did not have a statistically
significant clinical effect in patients with severe CAP (RR: 1.19; 95% CI: 0.99–1.42),
mechanical ventilation time (WMD: −
2.30; 95% CI: −
6.09–1.49). However, corticosteroids treatment was significantly associated with reduced
in-hospital mortality (RR: 0.49; 95% CI: 0.29–0.85), reduced length of hospital stay
(WMD: −
4.21; 95% CI: −
6.61 to −
1.81).
Conclusion
Corticosteroids adjuvant therapy in patients with severe CAP may reduce the rate of
in-hospital mortality, reduce the length of hospital stay, and reduce CRP levels.
Keywords
To read this article in full you will need to make a payment
Subscribe to The American Journal of Emergency Medicine
Already a print subscriber? Claim online access
Already an online subscriber? Sign in
Register: Create an account
Institutional Access: Sign in to ScienceDirect
References
- New perspectives on community-acquired pneumonia in 388,406 patients. Results from a nationwide mandatory performance measurement programme in healthcare quality.Thorax. 2009; 64: 1062-1069
- Patients with community acquired pneumonia admitted to European intensive care units: an epidemiological survey of the GenOSept cohort.Crit Care. 2014; 18: R58
- Severe community-acquired pneumonia as a cause of severe sepsis: data from the PROWESS study.Crit Care Med. 2005; 33: 952-961
- Efficacy and safety of corticosteroids for persistent acute respiratory distress syndrome.N Engl J Med. 2006; 354: 1671-1684
- Corticosteroids and community-acquired pneumonia.Clin Pulm Med. 2003; 10: 255-262
- Adjunct prednisone therapy for patients with community-acquired pneumonia: a multicentre, double-blind, randomised, placebo-controlled trial.Lancet. 2015; 385: 1511-1518
- Effect of corticosteroids on treatment failure among hospitalized patients with severe community-acquired pneumonia and high inflammatory response: a randomized clinical trial.JAMA. 2015; 313: 677-686
- Dexamethasone and length of hospital stay in patients with community-acquired pneumonia: a randomised, double-blind, placebo-controlled trial.Lancet. 2011; 377: 2023-2030
- Low-dose corticosteroid use and mortality in severe community-acquired pneumonia patients.Eur Respir J. 2015; 45: 463-472
- Adjunctive corticotherapy for community acquired pneumonia: a systematic review and meta-analysis.PLoS One. 2015; 10e0144032
- Adjunctive systemic corticosteroids for hospitalized community-acquired pneumonia: systematic review and meta-analysis 2015 update.Sci Rep. 2015; 5: 14061
- Effects of corticosteroids on severe community-acquired pneumonia in elderly-patients: a meta-analysis.Chin J Clin. 2014; 20: 3640-3645
- Corticosteroid therapy for severe community-acquired pneumonia: a meta-analysis.Respir Care. 2014; 59: 557-563
- Clinical efficacy of glucocorticoids in the treatment of severe community acquired pneumonia and its impact on CRP.J Clin Pulm Med. 2013; 18: 1171-1173
- Effect of corticosteroids on the clinical course of community-acquired pneumonia: a randomized controlled trial.Crit Care. 2011; 15: R96
- Efficacy of corticosteroids in community-acquired pneumonia: a randomized double-blinded clinical trial.Am J Respir Crit Care Med. 2010; 181: 975-982
- Efficacy of corticosteroids in the treatment of community-acquired pneumonia requiring hospitalization.Lung. 2007; 185: 249-255
- Application value of glucocorticoid for comprehensive treatment of acute respiratory distress syndrome induced by serious community acquired pneumonia.Clin Med Eng. 2015; 22: 57-58
- Hydrocortisone infusion for severe community-acquired pneumonia: a preliminary randomized study.Am J Respir Crit Care Med. 2005; 171: 242-248
- Hydrocortisone and tumor necrosis factor in severe community-acquired pneumonia. A randomized controlled study.Chest. 1993; 104: 389-392
- Corticosteroids and ICU course of community acquired pneumonia in Egyptian settings.Pharmacol Pharm. 2011; 2: 73-81
- Value of glucocorticoid steroids in the treatment of patients with severe community-acquired pneumonia complicated with septic shock.Chin Crit Care Med. 2016; 28: 780-784
- Effects of corticosteroids on severe community-acquired pneumonia: a meta-analysis.Dalian Med Univ. 2015;
- Efficacy and safety of corticosteroids for community-acquired pneumonia: a systematic review and meta-analysis.Chest. 2016; 149: 209-219
Article Info
Publication History
Published online: July 15, 2017
Accepted:
July 14,
2017
Received in revised form:
July 14,
2017
Received:
December 7,
2016
Footnotes
☆Conflict of interests: All authors declare that they have no conflict of interests.
☆Acknowledgments: None.
Identification
Copyright
© 2017 Elsevier Inc. All rights reserved.
