
Intubation rate of patients with hypoxia due to COVID-19 treated with awake proning: A meta-analysis
a b s t r a c t
Background: Awake Prone positioning (PP), or proning, is used to avoid intubations in hypoxic patients with COVID-19, but because of the disease’s novelty and constant evolution of treatment strategies, the efficacy of awake PP is unclear. We conducted a meta-analysis of the literature to assess the intubation rate among patients with COVID-19 requiring oxygen or noninvasive ventilatory support who underwent awake PP. Methods: We searched PubMed, Embase, and Scopus databases through August 15, 2020 to identify relevant ran- domized control trials, observational studies, and case series. We performed random-effects meta-analyses for the primary outcome of intubation rate. We used moderator analysis and meta-regressions to assess sources of heterogeneity. We used the standard and modified Newcastle-Ottawa Scales (NOS) to assess studies’ quality. Results: Our search identified 1043 articles. We included 16 studies from the original search and 2 in-press as of October 2020 in our analysis. All were observational studies. Our analysis included 364 patients; mean age was
56.8 (SD 7.12) years, and 68% were men. The intubation rate was 28% (95% CI 20%-38%, I2 = 63%). The mortality rate among patients who underwent awake PP was 14% (95% CI 7.4%-24.4%). Potential sources of heterogeneity were study design and setting (practice and geographic).
Conclusions: Our study demonstrated an intubation rate of 28% among hypoxic patients with COVID-19 who underwent awake PP. Awake PP in COVID-19 is feasible and practical, and more rigorous research is needed to confirm this promising intervention.
(C) 2021
The development of Acute respiratory distress syndrome , or an ARDS-like syndrome, has been described among the majority of pa- tients critically ill with COVID-19 and confers a high mortality rate, re- ported by some authors to surpass 90% [1-5]. The underlying pathophysiology of COVID-19 remains poorly understood. Using data from Seattle (Washington, USA) and Boston (Massachusetts, USA), re- searchers proposed that COVID-19 confers a type of “Pseudo-ARDS”
* Corresponding author at: 22 South Greene Street, Suite T3N45 Baltimore, MD 21021, USA.
E-mail addresses: [email protected] (S. Cardona), [email protected] (Q.K. Tran).
1 Please direct all reprint requests to Quincy K Tran, [email protected], Department of Emergency Medicine, University of Maryland School of Medicine, Baltimore, MD, United States of America
characterized by diffuse atelectasis without the underlying alveolar and endothelial damage as observed in patients with traditional ARDS [2,6]. Patients with respiratory distress associated with COVID-19 re- spond quickly and well to positive pressure ventilation with apparent high recruitability [7]. The poor outcomes reported in many patients with COVID-19 that required early intubation, and the opportunity for clinical improvement suggested by high recruitability, have led many clinicians to investigate the implementation of recruitment methods to avoid mechanical ventilation.
Prone positioning (PP), or proning, is a well-established and com- monly used treatment strategy for patients with severe ARDS: it has been shown to improve the P/F ratio-the ratio of partial pressure of ox- ygen (PaO2) to fraction of inspired oxygen (FiO2)-while reducing re- quired positive end-expiratory pressure , oxygen requirements, and ventilator-dependent days [8-11]. Additionally, when performed for more than 12 h per day, PP has been associated with a Mortality benefit in severe ARDS patients requiring mechanical ventilation
https://doi.org/10.1016/j.ajem.2021.01.058
0735-6757/(C) 2021
[8,9,12-15]. PP is thought to confer all of these benefits by decreasing transpulmonary pressure gradients and alleviating the compression of alveoli, thus reducing Ventilator-induced lung injury [15-17]. In the su- pine position, ventral alveoli may be overinflated by mechanical ventila- tion (leading to volutrauma and barotrauma), while more dorsal alveoli are compressed (atelectrauma) by the ventral lung as well as the heart and diaphragm [17-22]. Proning is thought to even the distribution of gravitational forces and aeration within the lung and reduce the pres- sure exerted by the heart and diaphragm, reducing barotrauma, atelectrauma, and ventilation/perfusion mismatch [11,13,15,17,18,23]. Proning further promotes aeration of the posterior and basal lung fields by limiting the motion of the anterior chest wall [13,19,20], and has been associated with an improvement of secretion clearance [18,22]. PP may have greater effects when utilized in the earlier stages of ARDS development, when alveolar collapse is more likely to be reversible [16,20,24].
The current literature reports highly variable rates of intubation for
patients with COVID-19 not undergoing awake PP, ranging from 55% to 88% [25-30]. The positive impact of proning on intubated patients with ARDS has led many to suggest applying this strategy to nonintubated awake patients [18,31,32]. Limited evidence collected to date of patients requiring respiratory support with supplemental oxy- gen, but not yet requiring mechanical ventilation, suggests that awake PP may improve oxygenation, prevent intubations, and improve patient outcomes [18,33]. However, the majority of the available evidence has been of relatively low quality, mostly in the form of case reports and small case series, due to COVID-19’s novelty and the immediate need for data. In this systematic review and meta-analysis, we sought to eval- uate the available evidence regarding the efficacy of awake PP and the prevalence of intubation in patients with COVID-19 undergoing awake PP.
We conducted this study in accordance with the 2015 PRISMA (Pre- ferred Reporting Items for Systematic Review and Meta-Analysis) state- ment [33]. We identified potentially eligible studies through a search of PubMed, Scopus, and Embase databases up through August 15, 2020. To include many potential studies, we used broad search terms: (covid-19 OR coronavirus OR sars-COV) AND (proning OR prone). Our study was not registered with the PROSPERO registry.
Given the dynamic development of data and the novelty of the disease state of interest, we included meeting and poster abstracts, case series, retrospective and prospective studies, and randomized and quasi-randomized trials in our analysis. To improve our study’s quality, power, and timeliness, we also included eligible in-press articles that became available while we were preparing the manuscript. We in- cluded studies of adult patients (age > 18 years) who underwent PP while awake and alert, prior to intubation and invasive mechanical ven- tilation. Studies were eligible regardless of the level of noninvasive oxy- gen support required by their included patients (no oxygen, low-flow oxygen by nasal cannula, high-flow nasal cannula [HFNC], or bilevel or continuous positive airway pressure [BiPAP or CPAP]).
We contacted authors of studies that met all inclusion criteria but did not report the rate of invasive mechanical ventilation. We excluded studies that were not in the English language, included nonhuman sub- jects, did not present original data (that is, any commentaries or re- views), or were case reports (due to their publication bias and because they would not reflect the true rate of intubation among proned patients). Studies were also excluded if they included pediatric patients, failed to implement PP prior to intubation, or did not report intubation rates.
Our team emailed the corresponding authors of 7 studies to request additional information or clarification of reported data. Two authors responded, but only one provided additional data.
We used Covidence (www.covidence.org; accessed 9 December 2020) to manage the references for our meta-analysis. Two authors in- dependently reviewed each title and abstract. A third author indepen- dently adjudicated any disagreements. Each title and abstract required 2 agreements to advance to full-text reviews. We used the same process for the full-text screening step.
-
- Outcomes
Our primary outcome of interest was the rate of endotracheal intu- bation and invasive mechanical ventilation among patients with COVID-19 undergoing awake PP. Secondary outcomes were the rate of intubation within 24 h of presentation and any mortality rate as re- ported by the authors.
-
- Quality assessment
Two authors evaluated each included study to determine study qual- ity, with disagreements resolved through discussion between the 2 and a third author. We assessed the quality of Observational cohort studies using the Newcastle-Ottawa Scale (NOS) [34] or the modified NOS
[35] for case series. The NOS assesses each study according to 3 domains(selection of the cohort, comparability of the groups, and quality of out- come), and awards a maximum of 9 points. High-quality studies have a score >= 7, whereas moderate- and low-quality studies have scores of 4-6 and <= 3, respectively. The modified NOS assesses the same 3 do- mains but awards a maximum of 5 points because of case series' limita- tions. As a result, no case series can achieve higher than low to moderate quality.
Interrater agreement was assessed using weighted kappa scores, with a score of <0.2 corresponding to poor agreement; 0.21-0.4, fair agreement; 0.41-0.6, moderate agreement; 0.61-0.8, good agreement; and 0.81-1.00, very good agreement. We assessed heterogeneity by using both the Q statistic and the I2 statistic. The Cochran Q statistic tests the null hypothesis that all studies in the analysis would share a common effect size, if the value of the Q statistic is less than or equal to the degree of freedom. The I2 statistic provides the percentage of total variance as a difference in effect size across studies.
-
- Data extraction
We extracted data into a standardized Excel spreadsheet (Microsoft Corp). We collected data regarding patient demographics (including age and comorbidities), initial vital signs, initial laboratory data (includ- ing blood gas analysis as well as inflammatory markers thought to be as- sociated with severity of COVID-19 [36]), radiographic findings, noninvasive ventilation (NIV) type and settings, time to NIV and proning, total proning hours, improvement in P/F ratio after proning, and intubation and mortality rates.
To ensure adequate interrater agreement, at the start of the project, the 3 authors who performed all subsequent data extraction extracted data from the same 6 studies. The third of these authors then ran kappa scores to assess interrater reliability for consistency in our data extraction. After this initial test to ensure acceptable interrater reliabil- ity, 2 authors proceeded to extract data for each study. Any conflict was discussed and resolved as a group.
-
- Statistical analysis
We selected a meta-analysis as our main inquiry into this clinical question due to the unique situation of the disease: the COVID-19 pan- demic has spread across multiple very different regions of the world over the course of almost a year. The practice of awake PP has been
utilized in several different practice and geographic settings during this time as well. By performing a meta-analysis and subgroup analyses, we hoped to assess and compare outcomes associated with the disease and this particular intervention across different global regions and time pe- riods. Due to the uncertainties of the disease and the process of awake PP, the performance of meta-regressions provided further ways to de- tect clinical factors associated with the outcome of interest, with the aim of providing clinicians with valuable information to guide clinical practice or future research.
We used random-effects models to measure the rate of outcomes across the pooled patient population. Any studies reporting 2 similar outcomes were eligible for random-effects meta-analysis. We expressed categorical variables as percentages and continuous variables as means. Since many authors did not report standard deviations for the means of their continuous variables, we did not report standard deviations in our results. For studies that reported medians and interquartile ranges, we converted median to mean and SD as previously described by Lou et al. [37]. We also performed subgroup analyses to identify potential sources of heterogeneity and possible differences between subgroups. We a priori defined categorical moderator variables, including study de- sign, World Health Organization region according to the country of study, months of publication (as all included studies were published in 2020), type of oxygen delivery devices used, and the number of pa- tients in each study. We performed histogram analysis of continuous variables before categorizing them into groups as needed, according to their frequency of distribution.
We used meta-regressions and continuous independent variables, as available from any study, to assess potential variables associated with endotracheal intubation and invasive mechanical ventilation. These continuous independent variables included age, percentage male, P/F ratio and respiratory rate oxygenation (ROX) index at triage, change in P/F ratio and ROX index between triage and earliest repeat, and num- ber of days proning. For studies that did not report P/F ratio or ROX index, we calculated the values from the reported components. The ROX index is a clinical prediction rule that estimates the likelihood of in- tubation in patients requiring HFNC in the management of hypoxemic respiratory failure, calculated from respiratory rate, oxygen saturation, and FiO2. Risk of intubation is low if ROX index is >=4.8 and high if ROX index is <=3.8 [38]. The P/F ratio assesses lung function in acute lung injury. A P/F ratio less than 300 suggests mild ARDS, a value <200 is suggestive of moderate ARDS, and a value <100 represents severe ARDS [38].
We also performed sensitivity analysis by using “remove-one study”
random-effects meta-analysis to assess the effect of each individual study on the overall effect size. We did not perform a funnel plot to as- sess publication bias in our study. Traditionally, a funnel plot is utilized to estimate whether the missing negative studies would change the in- terventions’ overall effect size [39]. Our meta-analysis only measured the prevalence of intubation, so tests for publication bias were not appli- cable. We performed our meta-analysis using the software Comprehen- sive Meta-Analysis (www.meta-analysis.com; accessed 9 December 2020).
Our electronic search identified 1043 studies. After reviewing 56 full-text articles, we included 16 studies from our original search in our analysis. We also reviewed and added 2 in-press articles that be- came available in October 2020, after our initial search query (Fig. 1). Five (28%) of our studies were prospective, and 13 were retrospective. The majority of the selected studies were case series (n = 13, 72%), and the remaining were cohort studies (Table 1). Four studies included a control group, and 3 of these reported our outcome of interest.
The kappa score for data extraction was 0.9 (95% CI 0.6-0.99), which demonstrated “very good” interrater agreement.
-
- Study quality
We assessed the quality of most studies included in our meta- analysis as low to moderate quality, with 4 studies (22%) graded as high quality (Table 1). The weighted kappa score for the study quality assessments was 0.62 (95% CI 0.4-0.83), which reflects good interrater agreement.
-
- Summary of studies
Our meta-analysis included a total of 364 patients with COVID-19 who underwent awake PP during their hospitalization (Table 2). One hundred and seven patients (29%) underwent awake PP in the emergency department, 73 (20%) in a non-intensive care setting (step-down, intermediate care unit, or hospital wards), and 26 (7%) in an intensive care unit (ICU); 87 (24%) patients were reported as a mix of ICU and non-ICU patients. The clinical setting was not reported in 71 patients. Our patient population’s mean age was 56.8 (SD 7.12), and 68% were men. The majority of the studies were from the European region (33%), followed by Region of the Americas and West- ern Pacific Region (28% each), and Eastern Mediterranean Region (11%).
Eight (44%) studies reported using a mixture of CPAP, HFNC, and low-flow nasal cannula for oxygen delivery and ventilatory support; 4 (22%) used CPAP; and 3 used HFNC. The remaining 3 studies did not re- port the type of oxygen delivery device used. Mean oxygen delivered was 50.8 l per minute and 70% FiO2 (SD 20.2).
Fifteen studies reported an initial (prior to awake PP) P/F ratio or the data needed to calculate it, and 12 studies reported repeat (after awake PP) values. Among these, the mean initial P/F ratio was 160.7 (SD 71.5) and mean repeat P/F ratio was 183.2 (SD 47.7). Eleven studies reported an initial (prior to awake PP) ROX index or its components, and 9 stud- ies reported repeat (after awake PP) values. Among these, the mean ini- tial ROX index was 8.8 (SD 3.7), and the mean repeat ROX index was 8.8 (SD 5.4).
-
- Primary outcome: prevalence of intubation
Out of the 364 patients with COVID-19 who underwent awake PP, our analysis identified an intubation rate of 28% (95% CI 20%-38%) (Fig. 2). The Q statistic was 45 with 17 degrees of freedom, and the P value was 0.001, which suggested that the effect sizes were different from the true effect size across the studies in our meta-analysis. The I2 statistic was 63%, which suggested that 63% of variance in the observed effects was due to variance in true effects and not to chance.
The prediction interval (Fig. 2) was between 8% and 64%, suggesting that 95% of comparable studies would report a rate of intubation from as low as 8% to as high as 64%. As a result, some future studies are expected to report a low intubation rate, while other studies would report a rela- tively high intubation rate.
-
-
- Subgroup analysis
-
When studies were grouped by World Health Organization region, we found a higher percentage of intubation seen in the Americas and European regions, 33% and 31% respectively, and a lower percentage in the Western Pacific and Eastern Mediterranean regions, 22% and 13% respectively (Table 3A). However, the overall difference between these groups was not statistically significant. (See Table 3B.)
When studies were grouped according to study design, we observed
similar rates of intubation per design, with prospective studies having less heterogeneity (Table 3A). Less heterogeneity was also seen in stud- ies with fewer than 10 patients, and these studies also had lower intuba- tion rates; but the overall difference among studies grouped by patient
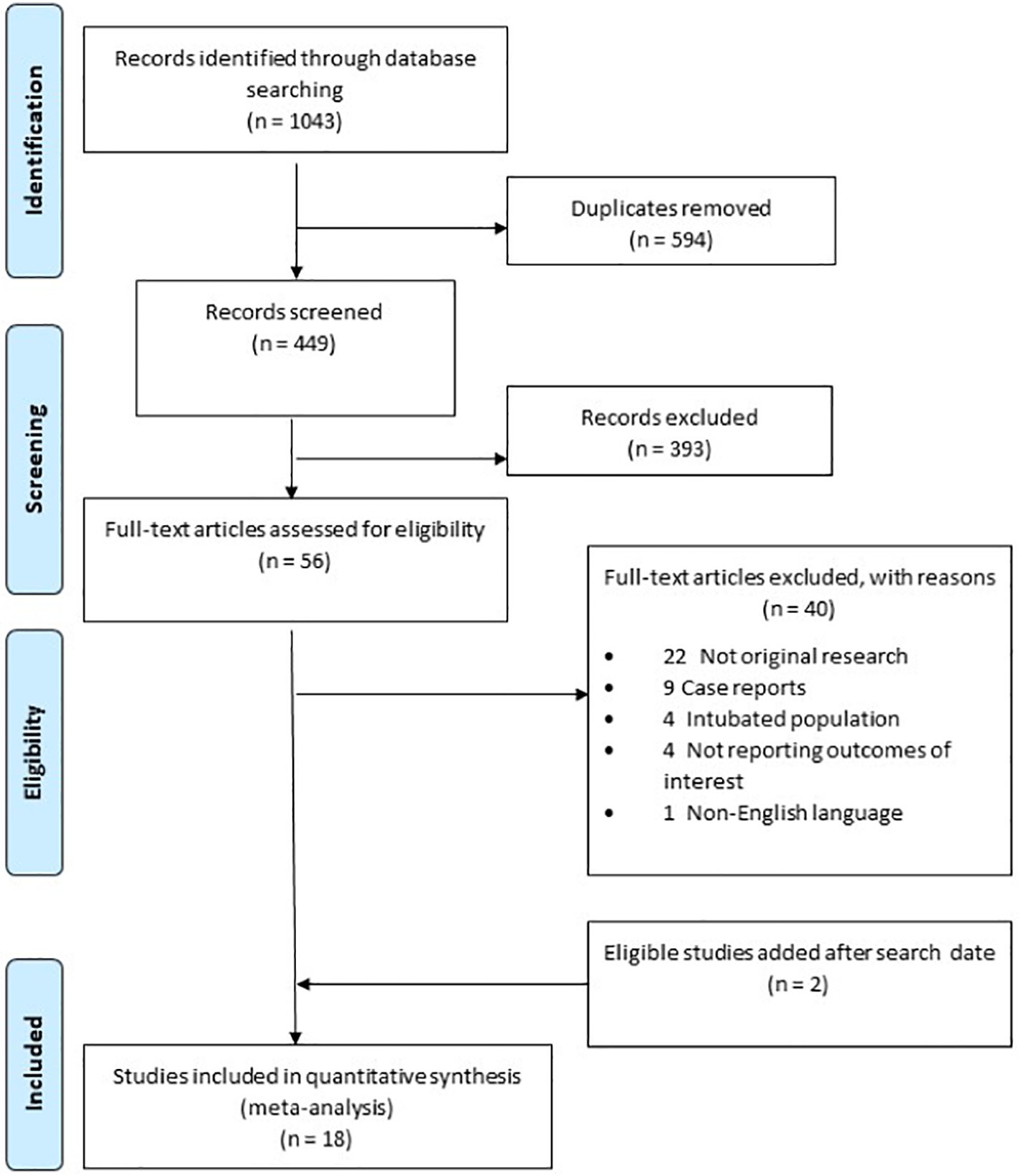
Fig. 1. PRISMA flow diagram for study selection.
Characteristics of studies included in meta-analysis
|
First author |
Month of publication |
Country and WHO region of study |
Study design |
Study type |
Clinical setting |
Study quality grading* |
|
Caputo [41] |
May |
USA; PAHO |
Prospective |
Cohort |
ED |
5 |
|
Cohen [42] |
July |
Israel; EMRO |
Retrospective |
Case series |
Not reported |
4 |
|
Coppo [43] |
June |
Italy; EURO |
Prospective |
Cohort |
ED/ICU/non-ICU |
6 |
|
Damarla [44] |
June |
USA; PAHO |
Retrospective |
Case series |
ICU |
5 |
|
Despres [45] |
May |
France; EURO |
Retrospective |
Case series |
ICU |
4 |
|
Elharrar [46] |
May |
France; EURO |
Prospective |
Case series |
Not reported |
5 |
|
Golestani-Eraghi [47] |
May |
Iran; EMRO |
Retrospective |
Case series |
ICU |
3 |
|
Huang [48] |
June |
Singapore; WRPO |
Retrospective |
Case series |
Not reported |
5 |
|
Jagan [25] |
October |
USA; PAHO |
Prospective |
Cohort |
Non-ICU/ICU |
7 |
|
Moghadam [49] |
May |
Iran; EMRO |
Retrospective |
Case series |
Non-ICU |
4 |
|
Ng [50] |
July |
Singapore; WRPO |
Retrospective |
Case series |
Non-ICU |
5 |
|
Padrao [26] |
October |
Brazil; PAHO |
Retrospective |
Cohort |
ED |
8 |
|
Ripoll-Gallardo [51] |
July |
Italy; EURO |
Retrospective |
Case series |
Non-ICU |
2 |
|
Sartini [52] |
May |
Italy; EURO |
Retrospective |
Case series |
Non-ICU |
5 |
|
Thompson [53] |
June |
USA; PAHO |
Retrospective |
Cohort |
Non-ICU |
8 |
|
Tu [54] |
May |
China; WRPO |
Retrospective |
Case series |
Not reported |
4 |
|
Xu [55] |
May |
China; WRPO |
Retrospective |
Case series |
Not reported |
5 |
|
Zang [27] |
July |
China; WRPO |
Prospective |
Case series |
Not reported |
8 |
Abbreviations: ED, emergency department; ICU, intensive care unit; PAHO, Pan American Health Organization; EURO, WHO European Region; WRPO, Regional Office for the Western Pa- cific; EMRO, Regional Office for the Eastern Mediterranean.
The Newcastle-Ottawa Scale (NOS) and modified NOS were used to assess the methodological quality of the included studies. High quality studies have a score >= 7, moderate and low quality studies have scores of 4-6 and <= 4 respectively*.
Patient characteristics
|
First author |
Number of proned patients |
Mean age |
Male n (%) |
BMI |
Initial P/F ratio |
Initial ROX index |
Oxygen delivery device (% patient use) |
Daily proning duration, h |
Total proning duration, h |
Repeat PF ratio |
Repeat ROX index |
Intubation in 24 h |
Any intubation |
Total death |
|
Caputo [41] |
50 |
59 |
30 (60%) |
NR |
108 |
11 |
NC (24%), |
NR |
NR |
197 |
NR |
13 |
18 |
NR |
|
NRBM (76%) |
||||||||||||||
|
Cohen [42] |
2 |
46 |
1 (50%) |
NR |
252 |
15 |
NC (50%), |
4 |
NR |
145 |
4 |
0 |
0 |
0 |
|
HFNC (50%) |
||||||||||||||
|
Coppo [43] |
47 |
57 |
44 (94%) |
28 |
181 |
8 |
CPAP (79%) |
3 |
21 |
193 |
6 |
NR |
13 |
5 |
|
Damarla [44] |
10 |
56 |
7 (70%) |
NR |
181 |
8 |
NC (50%), |
4 |
NR |
224 |
9 |
2 |
2 |
0 |
|
HFNC (40%) |
||||||||||||||
|
Despres [45] |
6 |
59 |
6 (100%) |
27 |
187 |
NR |
NC (66%), |
3 |
3 |
205 |
NR |
NR |
3 |
NR |
|
HFNC (33%) |
||||||||||||||
|
Elharrar [46] |
24 |
66 |
16 (67%) |
NR |
214 |
15 |
NC (67%), |
NR |
NR |
246 |
15 |
NR |
5 |
NR |
|
HFNC (33%) |
||||||||||||||
|
Golestani-Eraghi |
10 |
NR |
NR |
NR |
150 |
NR |
CPAP (100%) |
NR |
9 |
NR |
NR |
NR |
2 |
2 |
|
[47]
Huang [48] |
3 |
59 |
2 (67%) |
NR |
102 |
8 |
HFNC |
NR |
32 |
139 |
8 |
NR |
1 |
NR |
|
(100%) |
||||||||||||||
|
Jagan [25] |
40 |
56 |
8 (20%) |
31 |
NR |
NR |
NR |
NR |
NR |
NR |
NR |
NR |
4 |
0 |
|
Moghadam [49] |
10 |
41 |
7 (70%) |
NR |
NR |
NR |
NR |
NR |
NR |
NR |
NR |
0 |
0 |
0 |
|
Ng [50] |
10 |
60 |
8 (80%) |
NR |
310 |
NR |
NC (60%), |
5 |
25 |
NR |
NR |
NR |
1 |
1 |
|
VM (20%), |
||||||||||||||
|
HFNC (10%) |
||||||||||||||
|
Padrao [26] |
57 |
51 |
40 (70%) |
33 |
196 |
9 |
NC (34%), |
NR |
NR |
224 |
20 |
NR |
33 |
6 |
|
VM (5%), |
||||||||||||||
|
NRBM (61%) |
||||||||||||||
|
Ripoll-Gallardo |
13 |
66 |
11 (84%) |
NR |
115 |
5 |
CPAP (100%) |
NR |
7 |
166 |
6 |
3 |
9 |
7 |
|
[51]
Sartini [52] |
15 |
59 |
13 (86%) |
24 |
157 |
6 |
CPAP (100%) |
NR |
NR |
91 |
7 |
NR |
1 |
1 |
|
Thompson [53] |
25 |
67 |
18 (72%) |
31 |
15 |
8 |
NR |
4 |
8 |
NR |
NR |
NR |
12 |
3 |
|
Tu [54] |
9 |
51 |
4 (44%) |
NR |
86 |
NR |
HFNC |
2 |
10 |
135 |
NR |
NR |
2 |
NR |
|
(100%) |
||||||||||||||
|
Xu [55] |
10 |
50 |
5 (50% |
NR |
157 |
NR |
HFNC |
6 |
NR |
233 |
NR |
0 |
0 |
0 |
|
(100%) |
||||||||||||||
|
Zang [27] |
23 |
63 |
13 (56%) |
NR |
NR |
3.35 |
NC (68%), |
8 |
3 |
NR |
4 |
NR |
8 |
10 |
|
HFNC (22%) |
Abbreviations: BMI, body mass index; CPAP, continuous positive airway pressure; HFNC, high-flow nasal cannula; NC, nasal cannula; NR, not reported; NRBM, non-rebreather mask; P/F, partial pressure of oxygen / fraction of inspired oxygen; ROX, respiratory rate oxygenation; VM, venturi mask.
sample size was not statistically significant (this is likely reflecting
“small study effect”) (Table 3A).
The rate of intubation increased as the year 2020 progressed, with 24% in the months of April and May and 32% in the months of August to October (Table 3A); this difference was not statistically significant in subgroup analysis.
Our sensitivity analysis, using random-effects meta-analysis with one study removed, found the rate of any intubation 28% (95% CI 20%- 38%), suggesting that our results are robust and not disproportionately affected by any single study.
Six studies reported the number of patients with COVID-19 who underwent awake PP and were intubated within 24 h of presenta- tion (Fig. 3A). These studies report a total of 29 patients intubated during hospitalization, 18 (62%) of whom were intubated within 24 h of presentation, with an overall 24-h intubation rate of 22% (95% CI 14.7%-32.2%). The Q statistic was 3.5 with 5 degrees of freedom, and the P value was 0.61, which suggested that this effect size was similar across the studies in our meta-analysis. The I2 sta- tistic was 0%, suggesting low heterogeneity of effect size across the studies.
-
-
- Mortality
-
The pooled mortality rate for the 13 studies that reported Death rates was 14% (95% CI 7.4%-24.4%) (Fig. 3B). The Q statistic was 32 with 12 degrees of freedom, and the P value was 0.001, which suggested the true effect size was different across the studies in our meta-analysis. The I2 statistic was 62%, which suggested that 62% of variance in the ob- served effects was due to variance in true effect sizes.
- Discussion
Our meta-analysis investigated the need for invasive mechanical ventilation among patients with COVID-19 and hypoxia managed with awake PP in addition to supplemental oxygen or NIV and dem- onstrated an intubation rate of 28%, though with a wide prediction interval. The reported rates of intubation among patients with COVID-19 who have not undergone awake-PP have been highly var- iable (as has been the case with patients treated with awake-PP), ranging from 5% to 88% [25-30]. However, most of the rates reported among hypoxic patients with COVID-19 requiring supplemental oxy- gen or NIV (whose acuity more closely matches those who demon- strate a need for awake-PP) have been equal or higher than that identified in our study, but overall ranging from 11% to 88% [25-30]. Three of the studies included in this meta-analysis (Jagan, Padrao, and Zang) included a control group and reported intubation rates of 28% (unadjusted), 49%, and 11%, respectively [25-27]. Of note, al- though the rate of intubation reported by Zang et al. was lower (11%) in the non PP group than in the PP group (35%), patients
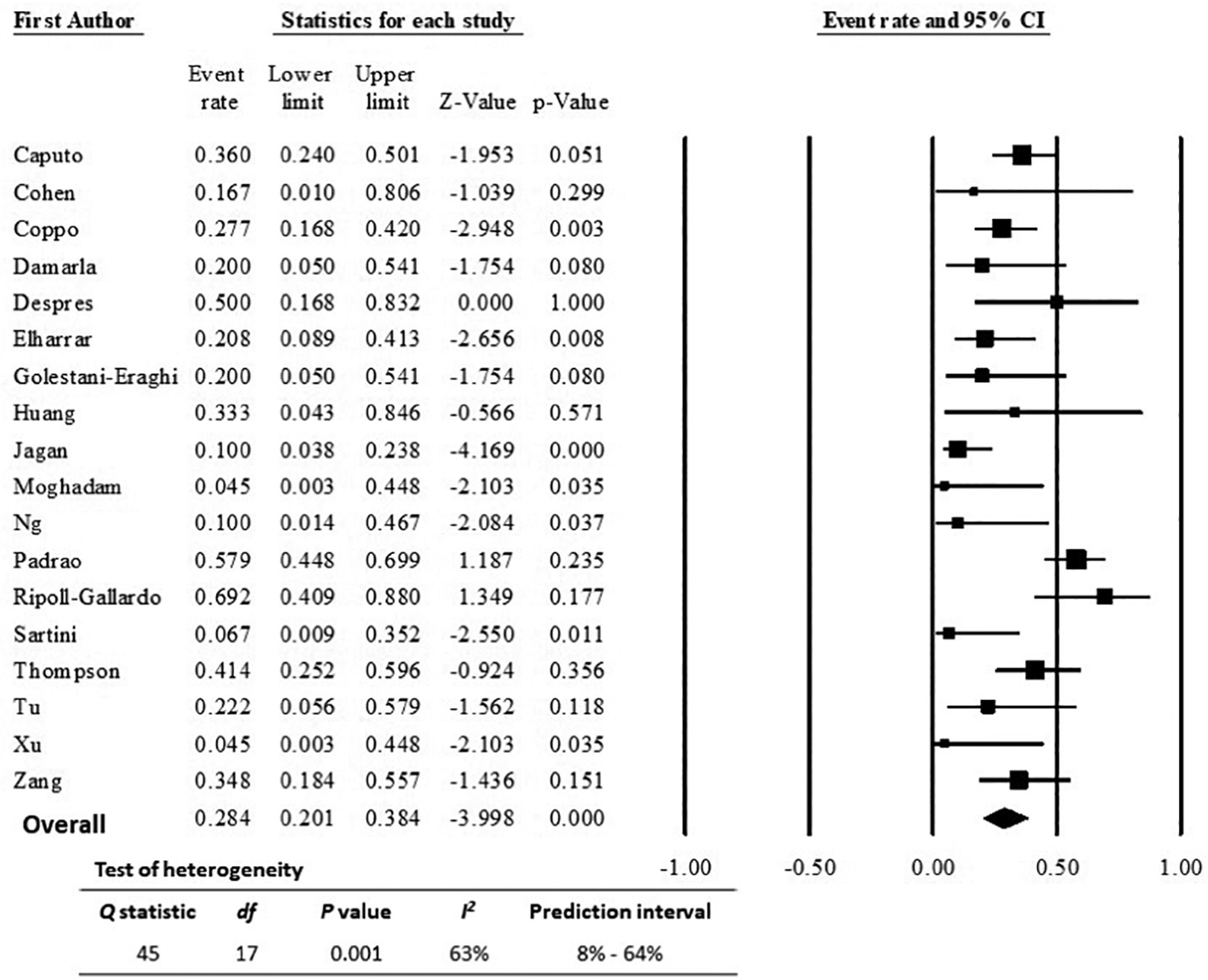
Fig. 2. Forest plot of random-effects meta-analysis for prevalence of any intubation during hospitalization among patients with COVID-19 undergoing awake proning.
who did not undergo PP, had a statistically significant longer length of stay (27 days compared to 8 days, p-value <0.01) and higher mor- tality rate (75.7% in comparison to 43.5%, p-value = 0.01) than those who did undergo awake PP.
The majority of the studies included in our meta-analysis are single- center, and it is thus difficult to generalize their results outside the spe- cific setting in which they were performed. By integrating their results, our meta-analysis provides insight into the expected results from a multi-center study. The heterogeneity of studies included in this analy- sis was high. One reason for this heterogeneity may be explained by our inclusion of studies from a variety of practice settings (emergency de- partments, general wards, and ICUs) as well as different countries
with potentially variable practice patterns, Health care resources, and types of Therapeutic treatment. However, our overall outcome did not change significantly when any single study was removed from the anal- ysis, suggesting that our results, while not precise, are robust and broadly applicable to a wide range of clinical settings.
Similar intubation rates were observed in both prospective and ret- rospective studies, though less heterogeneity was observed among pro- spective studies, as researchers might have had more control of the data collection and patient selection. Similarly, smaller studies-particularly case series-generally reported lower intubation rates (though the dif- ference in rates was not statistically significant) and were associated with less heterogeneity, implying the “small study effect,” in which
Results from moderator analyses using categorical variables and outcome of any intubation during hospital stay
|
Moderator variables |
Number of |
Any intubation |
95% CI |
Q |
df |
P value I2 Between group |
|||
|
studies |
(%) |
statistic |
comparison P value |
||||||
|
WHO region |
0.55 |
||||||||
|
EMRO |
2 |
13 |
3%-47% |
1 |
1 |
0.32 |
1% |
||
|
EURO |
6 |
31 |
17%-51% |
13 |
5 |
0.024 |
61% |
||
|
PAHO |
5 |
33 |
19%-51% |
21 |
4 |
0.001 |
80% |
||
|
WPRO |
5 |
22 |
9%-43% |
4 |
4 |
0.39 |
4% |
||
|
Study design |
0.81 |
||||||||
|
Prospective |
4 |
30 |
16%-49% |
2 |
3 |
0.55 |
0 |
||
|
Retrospective |
14 |
27 |
17%-40% |
42 |
13 |
0.001 |
69% |
||
|
Patient sample size |
<= 10 patients |
9 |
19 |
10%-35% |
6 |
8 |
0.59 |
0 |
0.36 |
|
11-39 patients |
5 |
34 |
19%-54% |
12 |
4 |
0.02 |
67% |
||
|
>= 40 patients |
4 |
32 |
18%-51% |
22 |
3 |
0.001 |
86% |
||
|
Month of publication |
0.84 |
||||||||
|
April-May 2020 |
7 |
24 |
11%-43% |
7 |
6 |
0.28 |
20% |
||
|
June-July 2020 |
9 |
29 |
17%-45% |
16 |
8 |
0.049 |
48% |
||
|
August-October 2020 |
2 |
32 |
12%-61% |
18 |
1 |
0.001 |
94% |
||
|
Types of oxygen delivery device |
0.63 |
||||||||
|
CPAP |
4 |
33 |
13%-61% |
10 |
2 |
0.006 |
80% |
||
|
HFNC |
3 |
19 |
5%-49% |
2 |
2 |
0.44 |
0 |
||
|
Mixed |
8 |
33 |
21%-46% |
19 |
8 |
0.015 |
58% |
||
Results from meta-regression measuring the associations between continuous variables and outcome of any intubation during hospital stay
|
Moderator variables |
Number of studies |
Correlation coefficient |
95% CI |
P value R2 I2 |
||
|
Age - years |
17 |
0.06 |
-0.02, 0.14 |
0.14 |
0 |
66% |
|
Percent of male patients |
17 |
1.7 |
-1.3, 5.01 |
0.3 |
0 |
65% |
|
BMI |
6 |
0.15 |
-0.13, 0.43 |
0.29 |
0.1 |
81% |
|
Initial P/F ratioa |
12 |
0 |
-0.01, -0.85 |
0.4 |
0 |
66% |
|
Delta P/F ratioa |
12 |
0.01 |
-0.01, 0.03 |
0.36 |
||
|
Initial ROX indexb |
-0.07 |
0.51 |
67% |
|||
|
11 |
-0.2, 0.08 |
0.45 |
||||
|
Delta ROX indexb |
9 |
0.1 |
-0.01, 0.2 |
0.06 |
||
|
Proning duration per day (hours) |
8 |
0.04 |
-0.19, 0.26 |
0.76 |
0 |
1% |
|
Total duration of proning (hours) |
9 |
-0.04 |
-0.09, 0.01 |
0.12 |
0.47 |
31% |
a,bMultivariable meta-regressions included both continuous variables. 95% CI, 95% confidence interval; BMI, body mass index; Delta, change between initial and repeat values of ROX index or P/F ratio; P/F ratio, PaO2 (partial pressure of oxygen)/FiO2 (fraction of inspired oxygen) ratio; ROX index, respiratory oxygen index.
small studies with favorable results were more preferentially reported and published [56].
Given the significant flux, rapid evolution, and uncertainty of treat- ment strategies for COVID-19, high heterogeneity in published studies
is to be expected. We observed that our meta-analysis’ heterogeneity was lower than that of other meta-analyses reporting prevalence of dis- ease related to COVID-19 [57,58]. Over the time period covered by the studies included in our analysis, popular and recommended treatment
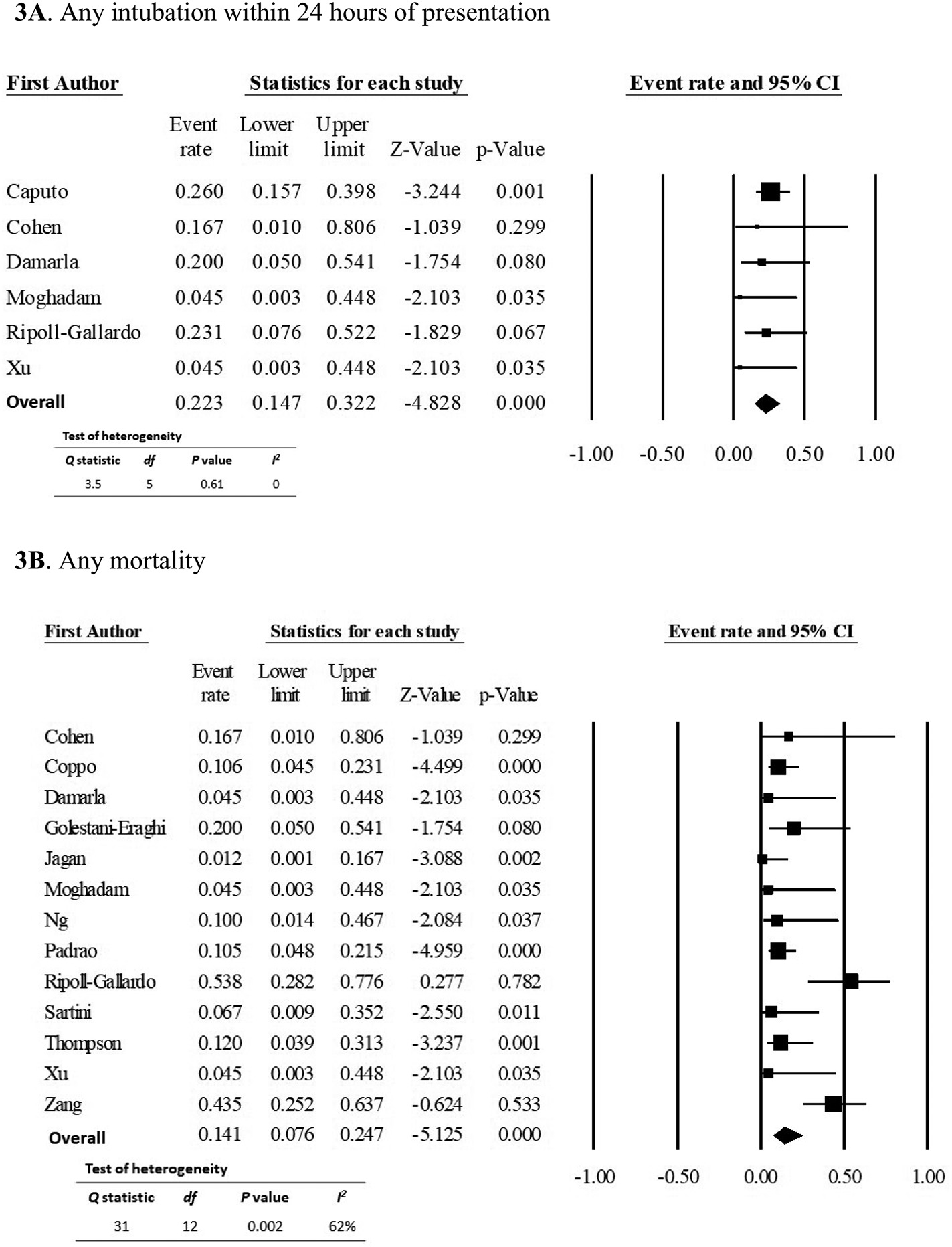
Fig. 3. Forest plot of secondary outcomes for COVID-19 patients undergoing awake proning 3A. Any intubation within 24 h of presentation 3B. Any mortality.
strategies have changed significantly, from the initial excitement and subsequent debunking of hydroxychloroquine and the confounding recommendations surrounding remdesivir [59], to the data supporting the early use of dexamethasone [60]. Our meta-analysis highlights the inherent difficulty in seeking precise results in a novel and continually shifting environment. However, our meta-analysis suggested that the prevalence of intubation was consistent across clinical settings and dif- ferent regions and through the uncertainty of therapeutic treatments. As a result, awake PP may be a promising intervention until results from further studies become available.
Our results further highlight the nuances involved in the clinical de- cision to intubate and the difficulty in capturing and reporting those nu- ances with objective measures. Specifically, P/F ratio and ROX index were not significantly associated with intubation rates in our multivar- iable meta-regressions. However, our exploratory results should not be taken to imply that either P/F ratio or the ROX index are not useful tools for assessing need for intubation among patients with COVID-19. There are a number of factors that can help explain these findings. We may not have enough studies within the meta-analysis to detect a significant as- sociation between intubation and P/F ratio or ROX index. Additionally, P/F ratio and ROX index are not the sole indicators of need for intubation in clinical practice. Most studies in our meta-analysis did not report ad- ditional important clinical factors regarding the decision to intubate, such as hemodynamic parameters, patients’ mental status and Work of breathing, signs of poor perfusion, and overall clinical picture. As such, our meta-regression may not show significant associations between P/F ratio or ROX index and intubation, without taking into account other clinical variables.
-
- Implications for future research
Our analysis suggests that awake PP is practical and feasible in vari- ous practice settings and across the globe. It highlights the need for mul- ticenter studies with adequate sample size, proper control groups, and more comprehensive reporting of additional therapeutic treatments. Such studies will have the potential to further elucidate not only the Clinical predictors, but also the utility, of awake PP. These well- designed studies would help clinicians to differentiate which patients might benefit most from early versus later intubation, and who might avoid intubation altogether through proning and NIV. Additionally, the complications reported by the studies included in our meta-analysis are relatively minor, mostly related to patient discomfort or increased cough. Therefore, our study suggests that the risks associated with awake PP are low, and the potential benefits are substantial enough to warrant more rigorous investigation.
Our analysis has many important limitations. Most of the included studies were of low to moderate quality, with no randomized trials and few including control groups. In addition, owing to the novelty of COVID-19 and the early push for data on treatment options and patient outcomes, as well as the Prolonged hospitalizations required by some patients, many studies reported outcomes over a predefined time pe- riod, rather than a patient’s entire hospital course. This limits our under- standing of the impact of awake PP on the patient’s full disease course. Furthermore, many included studies did not report data on key indi- cators of patients’ respiratory status, such as P/F ratios, ROX index, or chest X-ray or computed tomography (CT) results, which prevents full and accurate characterization of the patient population included. This in turn limits our ability to identify patients most or least likely to ben-
efit from awake PP.
Overall, this meta-analysis has served primarily as an exploration of available data and to highlight the need for more rigorous studies in the future. Because of the low quality of the studies available at this time, we agreed with the recommendations from the National Institute of
Health’s expert panel that awake PP may be trialed for hypoxic patients, but it should not be relied on as a Rescue therapy to avoid intubation altogether [61].
- Conclusion
Awake PP is a practical and promising intervention for patients re- quiring supplemental oxygen or NIV due to COVID-19 and may serve to prevent intubations. The intubation rate among such patients is esti- mated at approximately 30%. More rigorous studies are needed to con- firm this observation and further elucidate which patients might benefit most from awake proning to avoid intubation.
Source of funding
This research did not receive any specific grant from funding agen- cies in the public, commercial, or not-for-profit sectors.
Authors’ contributions
Conceptualization: QKT, BS, DM, JD, SC, RA.
Data collection: RA, SC, JD, MR, VB, IY, FY, BS, DM, QKT.
Data quality and data analysis: RA, SC, JD, MR, VB, IY, FY, QKT. Manuscript preparation: RA, SC, JD, QKT.
Critical revision of manuscript: RA, SC, JD, MR, VB, IY, FY, BS, DM, QKT.
Abbreviation: PRISMA, preferred reporting items for systematic re- views and meta-analyses.
Adapted from [40].
Declaration of Competing Interest
The authors declare no conflict of interest.
Acknowledgment
Deborah M. Stein, ELS, provided language editing of the manuscript.
References
- Arentz M, Yim E, Klaff L, et al. Characteristics and outcomes of 21 critically ill patients with COVID-19 in Washington state. JAMA. 2020;323(16):1612. https://doi.org/10. 1001/jama.2020.4326.
- Bhatraju PK, Ghassemieh BJ, Nichols M, et al. Covid-19 in critically ill patients in the Seattle region — case series. N Engl J Med. 2020;382(21):2012-22. https://doi.org/ 10.1056/NEJMoa2004500.
- Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395(10223):507-13. https://doi.org/10.1016/S0140-6736(20)30211-
7.
- Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020;323
(11):1061. https://doi.org/10.1001/jama.2020.1585.
- Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpa- tients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020; 395(10229):1054-62. https://doi.org/10.1016/S0140-6736(20)30566-3.
- Ziehr DR, Alladina J, Petri CR, et al. Respiratory pathophysiology of mechanically ven- tilated patients with COVID-19: a cohort study. Am J Respir Crit Care Med. 2020;201 (12):1560-4. https://doi.org/10.1164/rccm.202004-1163LE.
- Farkas J. PulmCrit - is COVID-19 ARDS, pseudoARDS, L, or H? physiology data from Bostonhttps://emcrit.org/pulmcrit/covid-pseudoards/;; 1 May 2020 [accessed 21
November 2020].
- Bloomfield R, Noble DW, Sudlow A. Prone position for acute respiratory failure in adults. Cochrane Database Syst Rev. 2015;11:CD008095. https://doi.org/10.1002/ 14651858.CD008095.pub2.
- Guerin C, Reignier J, Richard J-C, et al. Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 2013;368(23):2159-68. https://doi.org/10.1056/ NEJMoa1214103.
- Scaravilli V, Grasselli G, Castagna L, et al. Prone positioning improves oxygenation in spontaneously breathing Nonintubated patients with hypoxemic acute respiratory failure: a retrospective study. J Crit Care. 2015;30(6):1390-4. https://doi.org/10. 1016/j.jcrc.2015.07.008.
- van Meenen DM, Roozeman J-P, Serpa Neto A, et al. Associations between changes in oxygenation, dead space and driving pressure induced by the first prone position
session and mortality in patients with acute respiratory distress syndrome. J Thorac Dis. 2019;11(12):5004-13. https://doi.org/10.21037/jtd.2019.12.38.
- Abroug F, Ouanes-Besbes L, Dachraoui F, Ouanes I, Brochard L. An updated study- level meta-analysis of Randomised controlled trials on proning in ARDS and acute lung injury. Crit Care. 2011;15(1):R6. https://doi.org/10.1186/cc9403.
- Beitler JR, Shaefi S, Montesi SB, et al. Prone positioning reduces mortality from acute respiratory distress syndrome in the low tidal volume era: a meta-analysis. Intensive Care Med. 2014;40(3):332-41. https://doi.org/10.1007/s00134-013-3194-3.
- Hu S, He H, Pan C, et al. The effect of prone positioning on mortality in patients with acute respiratory distress syndrome: a meta-analysis of randomized controlled tri- als. Crit Care. 2014;18(3):R109. https://doi.org/10.1186/cc13896.
- Kallet RH. A comprehensive review of prone position in ARDS. Respir Care. 2015;60 (11):1660-87. https://doi.org/10.4187/respcare.04271.
- Albert RK, Keniston A, Baboi L, Ayzac L, Guerin C. Prone position-induced improve- ment in Gas exchange does not predict improved survival in the acute respiratory distress syndrome. Am J Respir Crit Care Med. 2014;189(4):494-6. https://doi.org/ 10.1164/rccm.201311-2056LE.
- Papazian L, Aubron C, Brochard L, et al. Formal guidelines: management of acute re- spiratory distress syndrome. Ann Intensive Care. 2019;9(1):69. https://doi.org/10. 1186/s13613-019-0540-9.
- Bamford P, Benteley A, Dean J, Whitmore D, Wilson-Baig N. ICS guidance for prone positioning of the conscious COVID patient 2020 [Internet]. Intensive Care Society. 2020:3-4 [cited 10 December 2020]. Available from: https://emcrit.org/wp- content/uploads/2020/04/2020-04-12-Guidance-for-conscious-proning.pdf.
- Gattinoni L, Busana M, Giosa L, Macri M, Quintel M. Prone positioning in acute respi- ratory distress syndrome. Semin Respir Crit Care Med. 2019;40(01):94-100. https:// doi.org/10.1055/s-0039-1685180.
- Gattinoni L, Taccone P, Carlesso E, Marini JJ. Prone position in acute respiratory dis- tress syndrome. Rationale, indications, and limits. Am J Respir Crit Care Med. 2013; 188(11):1286-93. https://doi.org/10.1164/rccm.201308-1532CI.
- Albert RK, Hubmayr RD. The prone position eliminates compression of the lungs by the heart. Am J Respir Crit Care Med. 2000;161(5):1660-5. https://doi.org/10.1164/ ajrccm.161.5.9901037.
- Scholten EL, Beitler JR, Prisk GK, Malhotra A. Treatment of ARDS with prone position- ing. Chest. 2017;151(1):215-24. https://doi.org/10.1016/j.chest.2016.06.032.
- Sztajnbok J, Maselli-Schoueri JH, Cunha de Resende Brasil LM, et al. Prone position- ing to improve oxygenation and relieve respiratory symptoms in awake, spontane- ously breathing non-intubated patients with COVID-19 pneumonia. Respir Med Case Rep. 2020;30:101096. https://doi.org/10.1016/j.rmcr.2020.101096.
- Meng L, Qiu H, Wan L, et al. Intubation and ventilation amid the Covid-19 outbreak.
Anesthesiology. 2020;132(6):1317-32. https://doi.org/10.1097/ALN.
- Jagan N, Morrow LE, Walters RW, et al. The POSITIONED study: prone positioning in nonventilated coronavirus disease 2019 patients-a retrospective analysis. Crit Care Explor. 2020;2(10):e0229. https://doi.org/10.1097/CCE.0000000000000229.
- Padrao EMH, Valente FS, Besen BAMP, et al. Awake prone positioning in COVID-19 hypoxemic respiratory failure: exploratory findings in a single-center retrospective cohort study. Acad. Emerg. Med. Epub 27 October 2020. doi:https://doi. org/10.1111/acem.14160.
- Zang X, Wang Q, Zhou H, Liu S, Xue X. COVID-19 early prone position study group. Efficacy of early prone position for COVID-19 patients with severe hypoxia: a single-center prospective cohort study. Intensive Care Med. 2020;46(10):1927-9. https://doi.org/10.1007/s00134-020-06182-4.
- Carrillo Hernandez-Rubio J, Sanchez-Carpintero Abad M, Yordi Leon A, et al. Out- comes of an intermediate respiratory care unit in the COVID-19 pandemic. PLoS One. 2020;15(12). https://doi.org/10.1371/journal.pone.0243968 e0243968. Pub- lished 2020 Dec 16.
- Grasselli G, Zangrillo A, Zanella A, et al. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy region, Italy. JAMA. 2020;323(16):1574-81. https://doi.org/10.1001/jama.2020.5394.
- Yang X, Yu Y, Xu J, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observa- tional study [published correction appears in lancet Respir med. 2020 Apr;8(4):e26]. Lancet Respir Med. 2020;8(5):475-81. https://doi.org/10.1016/S2213-2600(20) 30079-5.
- Dondorp AM, Hayat M, Aryal D, Beane A, Schultz MJ. Respiratory support in COVID- 19 patients, with a focus on resource-limited settings. Am J Trop Med Hyg. 2020;102 (6):1191-7. https://doi.org/10.4269/ajtmh.20-0283.
- Elkattawy S, Noori M. A case of improved oxygenation in SARS-CoV-2 positive pa- tient on nasal cannula undergoing prone positioning. Respir Med Case Rep. 2020; 30:101070. https://doi.org/10.1016/j.rmcr.2020.101070.
- Moher D, Shamseer L, Clarke M, et al. Preferred reporting items for systematic re- view and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4
- Wells G, Shea B, O’Connell D, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. http://www.ohri.ca/ programs/clinical_epidemiology/oxford.asp;. [accessed 2 August 2019].
- Murad MH, Sultan S, Haffar S, Bazerbachi F. Methodological quality and synthesis of case series and case reports. BMJ Evid-Based Med. 2018;23(2):60-3. https://doi.org/ 10.1136/bmjebm-2017-110853.
- Zeng F, Huang Y, Guo Y, et al. Association of inflammatory markers with the severity of COVID-19: a meta-analysis. Int J Infect Dis. 2020;96:467-74. https://doi.org/10. 1016/j.ijid.2020.05.05532425643. PMC7233226.
- Luo D, Wan X, Liu J, Tong T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res. 2018;27 (6):1785-805. https://doi.org/10.1177/0962280216669183.
- Villar J, Perez-Mendez L, Blanco J, et al. A universal definition of ARDS: the PaO2/FiO2 ratio under a standard ventilatory setting-a prospective, multicenter validation study. Intensive Care Med. 2013;39(4):583-92. https://doi.org/10.1007/s00134- 012-2803-x.
- Borenstein M. Common mistakes in meta-analysis and how to avoid them. Biostat: Englewood (NJ); 2019.
- Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6
(7). https://doi.org/10.1371/journal.pmed1000097 e1000097.
- Caputo ND, Strayer RJ, Levitan R. Early self-proning in awake, non-intubated patients in the emergency department: a single ED’s experience during the COVID-19 pan- demic. Acad Emerg Med. 2020;27(5):375-8. https://doi.org/10.1111/acem.13994.
- Cohen D, Wasserstrum Y, Segev A, et al. Beneficial effect of awake prone position in hypoxaemic patients with COVID -19: case reports and literature review. Intern Med
J. 2020;50(8):997-1000. https://doi.org/10.1111/imj.14926.
- Coppo A, Bellani G, Winterton D, et al. Feasibility and physiological effects of prone positioning in non-intubated patients with acute respiratory failure due to COVID- 19 (PRON-COVID): a prospective cohort study. Lancet Respir Med. 2020;8(8): 765-74. https://doi.org/10.1016/S2213-2600(20)30268-X.
- Damarla M, Zaeh S, Niedermeyer S, et al. Prone positioning of nonintubated patients with COVID-19. Am J Respir Crit Care Med. 2020;202(4):604-6. https://doi.org/10. 1164/rccm.202004-1331LE.
- Despres C, Brunin Y, Berthier F, Pili-Floury S, Besch G. Prone positioning combined with high-flow nasal or conventional oxygen therapy in severe COVID-19 patients. Crit Care. 2020;24(1):256. https://doi.org/10.1186/s13054-020-03001-6.
- Elharrar X, Trigui Y, Dols A-M, et al. Use of prone positioning in nonintubated pa- tients with COVID-19 and hypoxemic acute respiratory failure. JAMA. 2020;323
(22):2336. https://doi.org/10.1001/jama.2020.8255.
- Golestani-Eraghi M, Mahmoodpoor A. Early application of prone position for man- agement of Covid-19 patients. J Clin Anesth. 2020;66:109917. https://doi.org/10. 1016/j.jclinane.2020.109917.
- Huang C-F, Tay CK, Zhuang Y-F, Liu J, Sewa DW. Rationale and significance of patient selection in awake prone positioning for COVID-19 pneumonia. Eur Respir J. 2020;56 (3):2002173. https://doi.org/10.1183/13993003.02173-2020.
- Moghadam VD, Shafiee H, Ghorbani M, Heidarifar R. Prone positioning in manage- ment of COVID-19 hospitalized patients. Braz J Anesthesiol Engl Ed. 2020;70(2): 188-90. https://doi.org/10.1016/j.bjane.2020.05.001.
- Ng Z, Tay WC, Ho CHB. Awake prone positioning for non-intubated oxygen depen- dent COVID-19 pneumonia patients. Eur Respir J. 2020;56(1):2001198. https://doi. org/10.1183/13993003.01198-2020.
- Ripoll-Gallardo A, Grillenzoni L, Bollon J, Della Corte F, Barone-Adesi F. Prone posi- tioning in non-intubated patients with COVID-19 outside of the intensive care unit: more evidence needed. Disaster Med Public Health Prep Epub. 27 July 2020: 1-3. https://doi.org/10.1017/dmp.2020.267.
- Sartini C, Tresoldi M, Scarpellini P, et al. Respiratory parameters in patients with COVID-19 after using noninvasive ventilation in the prone position outside the in- tensive care unit. JAMA. 2020;323(22):2338. https://doi.org/10.1001/jama.2020. 7861.
- Thompson AE, Ranard BL, Wei Y, Jelic S. Prone positioning in awake, nonintubated patients with COVID-19 hypoxemic respiratory failure. JAMA Intern Med. 2020; 180(11):1537. https://doi.org/10.1001/jamainternmed.2020.3030.
- Tu G-W, Liao Y-X, Li Q-Y, et al. Prone positioning in high-flow nasal cannula for COVID-19 patients with severe hypoxemia: a pilot study. Ann Transl Med. 2020;8
(9):598. https://doi.org/10.21037/atm-20-3005.
- Xu Q, Wang T, Qin X, Jie Y, Zha L, Lu W. Early awake prone position combined with high-flow nasal oxygen therapy in severe COVID-19: a case series. Crit Care. 2020;24
- Zhang Z, Xu X, Ni H. Small studies may overestimate the effect sizes in critical care meta-analyses: a meta-Epidemiological study. Crit Care. 2013;17(1):R2. https:// doi.org/10.1186/cc11919.
- Chen Y-T, Shao S-C, Hsu C-K, Wu I-W, Hung M-J, Chen Y-C. Incidence of acute kidney injury in COVID-19 infection: a systematic review and meta-analysis. Crit Care. 2020;24(1):346. https://doi.org/10.1186/s13054-020-03009-y.
- Grant MC, Geoghegan L, Arbyn M, et al. The prevalence of symptoms in 24,410 adults infected by the novel coronavirus (SARS-CoV-2; COVID-19): a systematic re- view and meta-analysis of 148 studies from 9 countries. PLoS One. 2020;15(6): e0234765. https://doi.org/10.1371/journal.pone.0234765.
- WHO Solidarity trial consortium, Pan H, Peto R, et al. Repurposed antiviral drugs for COVID-19 -interim WHO SOLIDARITY trial results. medRxiv 2020.10.15.20209817 [Preprint]. Oct 15 2020 [cited 10 December 2020]: [17 p.]. https://doi. org/10.1101/2020.10.15.20209817v1
- Horby P, Lim WS, et al, RECOVERY Collaborative Group. Dexamethasone in hospital- ized patients with Covid-19 — preliminary report. N Engl J Med Epub. 17 July 2020. https://doi.org/10.1056/NEJMoa2021436 NEJMoa2021436.
- National Institutes of Health. COVID-19 treatment guidelines: care of critically ill pa- tients with COVID-19https://www.covid19treatmentguidelines.nih.gov/critical- care/;; 8 October 2020 [accessed 1 December 2020].