
False-positive urine pregnancy test in a woman with adenomysosis
Case Report
False-positive urine pregnancy test in a woman with adenomysosis
Abstract
We present a case of a 39-year-old woman presenting to the emergency department with persistent Vaginal bleeding with myoma and endometrium thickness. The qualitative urine human chorionic gonadotropin (hCG) showed positive result, however, the quantitative serum hCG had negative result. The negative serum hCG result suggests that the false- positive result was not caused by elevated circulating hCG. According to the urine hCG one-step pregnancy device, 1 mg/dL of hemoglobin may not interference the pregnancy result. Nevertheless, we found that the hemoglobin level was 40 mg/dL in the urine specimen. We designed a in vitro experiment to evaluate the effects of hemoglobin on urine pregnancy test. The concentrations of hemoglobin from 5 to 500 mg/dL did not yield a positive urine pregnancy test. On the basis of our findings, the false positive pregnancy test was not caused by hemoglobin. It is important to confirm a suspected false-positive urine hCG test using a quantitative serum hCG test. Although it is not certain the mechanism for false positive reaction in this peculiar sample, the ACON urine hCG one-step pregnancy will occasionally yield a false-positive result in this class of patients.
Herein, we report a 39-year-old woman (gravida 0, para 0) who presented to the emergency department due to persistent vaginal bleeding. Medication for myoma was prescribed for vaginal bleeding in other hospital on September 2008. She was found to have hypermenorrhea with massive blood clot, according to the gynecologic service. Laboratory results showed white blood cell count of 3.50 x 103/uL (Reference interval, 4.00-10.0 x 103/uL), hemoglobin level of 7.1 g/dL (reference interval, 12-16 g/dL), hematocrit of 20.8% (reference interval, 37%-48%), and platelet count of 124,000/uL (reference interval: 150,000-350,000/uL). The serum chemistry was unremarkable. Urine routine analysis showed red blood cell (3+), white blood cells (1+), and protein (2+). Urine sediment revealed Red blood cell count of 25 to 50/high-power field (HPF), white blood cell count of 25 to 50/HPF, epithelial cell count of 5 to 10/HPF, and bacteria (2+). We repeated the centrifugation twice (1500

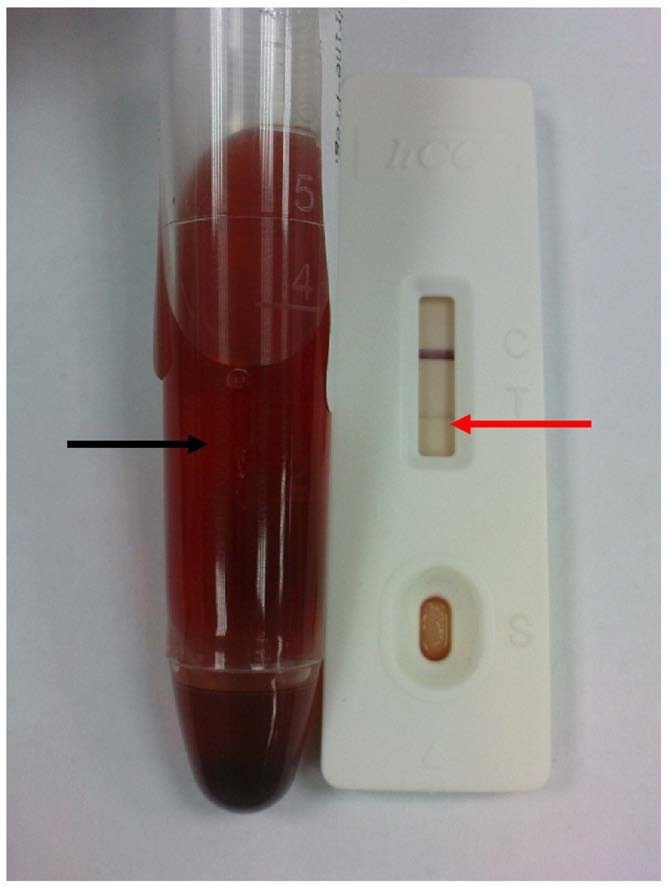
Fig. 1 The appearance of urine specimen is still reddish after centrifugation twice (black arrow). The result did yield a visible band in the result window (red arrow).
revolutions per minute, 10 minutes) because the appearance of urine specimen was bloody before urine pregnancy test, but the supernatant was still reddish (Fig. 1, red arrow). During her admission in our hospital for 4 days, sonography showed a left ovarian cyst (3.21 cm x 2.63 cm), small myoma (9.2 cm x 5.99 cm x 8.04 cm) and endometirum thickness. The abnormal bleeding is caused by endometrium thickness by adenomysosis. The abnormal bleeding is caused by endometrium thickness by adenomysosis. On the other hand, the biopsy of endometrium tissue determined that the polypoid lesion was supported by fibrovascular core and covered by endometrial gland with focal tubal metaplasia.
0735-6757/$ – see front matter (C) 2009
1019.e6 Case Report
In this case, the qualitative urine human chorionic gonadotropin (hCG) showed positive result (the result did yield a visible band in the result window) (Fig. 1, red arrow); however, the quantitative serum hCG had negative result (0.15 U/L; reference interval, b0.5-2.90 U/L). Therefore, the negative serum hCG result suggests that the false-positive result was not caused by elevated circulating hCG. According to the manufacturer’s information for the Acon urine hCG one-step pregnancy device (format, FHC-102), 1 mg/dL of hemoglobin may not interfere with the pregnancy result. Nevertheless, we found that the hemoglobin level was
40 mg/dL in the urine specimen using Coulter LH 750 hematology analyzer (Beckman Coulter Inc, Fullerton, Calif). To elucidate the effect of hemoglobinuria on urine pregnancy test, therefore, an in vitro experiment was designed to evaluate the effects of hemoglobin on urine pregnancy test. Red blood cells were lysed by 3 cycles of freeze-thaw. After red blood cell lysis by freeze-thaw, we centrifuged and then diluted the supernatant, in series, with urine obtained from a normal male individual. The concentrations of hemoglobin from 5 to 500 mg/dL (5, 10,
20, 50, 100, 200, 300, 400 and 500 mg/dL, respectively) did not yield a positive urine pregnancy test. On the basis of our findings, the false-positive pregnancy test was not caused by hemoglobin. Therefore, we suspected that other hCG molecules (e.g., ?-core fragments) might be responsible for their false-positive pregnancy tests.
Human chorionic gonadotropin is a glycoprotein com- posed of 2 dissimilar subunits, ? and ? subunits, held together by charge interactions. Both subunits are needed for biological activity and are common to other hormones (e.g., thyroid-stimulating hormone, luteinizing hormone, and follicle-stimulating hormone); however, the ?-subunit deter- mines the specificity of the biological action of the hormones containing these subunits [1]. In the circulation, the bulk of the hCG molecules exist as intact hormone (ie, ?–? dimer) with only small amounts of free ? and ? subunits. In urine, however, a large fraction of the immunoreactivity of hCG is due to a metabolic breakdown product of hCG, commonly known as ?-core fragment [2]. This fragment is believed to be a renal degradation product of intact hCG and free ?-subunit [3]. Although this fragment lacks the unique 30-amino acid carboxyl-terminal peptide of the ?-subunit of intact hCG, it retains conformational immunologic determinants in the urine of pregnant women and some women with various types of cancer sufficient to react with the hCG antibodies used in urine pregnancy tests. Moreover, ?-core fragment is virtually undetectable in serum using currently available serum hCG assays [4]. Using Sephadex G100 size exclusion chromatography, Papapetrou and Nicopoulou [5] reported that hCG ?-core fragment was present in the urine of patients with uterine cervix, colon, esophageal, or ovarian cancer.
Abnormal vaginal bleeding is the most common symptom experienced by women when they have a gynecologic cancer. Heavy periods, bleeding between periods, and
bleeding during and after sex are all considered abnormal vaginal bleeding and are symptoms of gynecologic cancer. The symptom of abnormal vaginal bleeding is linked to cervical cancer, uterine cancer, and ovarian cancer [6]. Besides, bleeding may also result from age-related thinning of the vagina thinning or thickening (hyperplasia) of the lining of the uterus, or thyroid disorders also can cause menstrual periods to be irregular, to be heavy, and occur more frequently or to occur less frequently. Regarding the uterine myoma, it is a benign cancer developed of muscular flat fibers that also contains conjunctive tissue in variable quantities as support element. The most common form of menstrual alterations in the myoma is the hypermenorrhea or menorrhagia. Our previous study [7] pointed out the need to be aware of colonic or cervical cancer as a potential cause of a false-positive urine pregnancy test in women with these conditions who are undergoing pregnancy screening using a urine hCG test. Therefore, we should follow up this patient in the future for early detection of cancer.
Determination of pregnancy status is important in the workup of a woman presenting with vaginal bleeding or lower abdominal pain. Women with these symptoms should be screened for pregnancy using a urine pregnancy test, especially, before undergoing an x-ray procedure. Clinical decisions regarding additional diagnostic testing should be based upon the results of the urine pregnancy test and knowledge of those conditions that can cause false-positive Screening tests for hCG in urine and serum, including the presence of serum human antimouse antibodies and diseases (e.g., colonic or cervical cancer) associated with excretion of hCG into the urine. A number of preanalytical conditions, other than pregnancy, including trophoblastic disease and certain nontrophoblastic neoplasms (e.g., testicular tumors, prostate cancer, breast cancer, and Lung cancer) can cause elevated serum levels of hCG that are then excreted into the urine [8,9]. False-positive urine hCG results have also been reported in patients with nephritic range proteinuria and Tubo-ovarian abscess [10,11]. Analytical causes of false- positive, or false-negative, urine hCG tests include human or technical error in the performance and/or interpretation of the test results.
A false-positive urine pregnancy test may place a patient at risk for unnecessary treatment. It is important to confirm a suspected false-positive urine hCG test using a quantitative serum hCG test. Although the mechanism for false positive reaction in this peculiar sample is not certain, the ACON urine hCG one step pregnancy device occasionally yields a false-positive result in this class of patient.
Tze Kiong Er PhD
Graduate Institute of Medicine
College of Medicine Kaohsiung Medical University
Kaohsiung, Taiwan Department of Laboratory Medicine Kaohsiung Medical university hospital
Kaohsiung, Taiwan
References
1019.e7
E-mail address: [email protected]
Chein-Hua Chiang Bin Hong Cheng Fu Jung Hong
Department of Laboratory Medicine Kaohsiung Medical University Hospital
Kaohsiung, Taiwan
Ching Ping Lee Division of Hematology-Oncology Department of Internal Medicine Kaohsiung Medical University Hospital
Kaohsiung, Taiwan
Miguel Angel Ruiz Gines MD Department of Pathology and Laboratory Medicine Hospital Virgen de la Salud (Toledo), Spain
Tze Kiong Er, Chein-Hua Chiang, and Miguel Angel Ruiz Gines contribute equally to this article.
doi:10.1016/j.ajem.2008.12.023
- Wu J, Nakamura R. Human circulating tumor markers. Current concepts and clinical applications. IL: American Society for Clinical Pathology; 1997. p. 127-76.
- Davison CM, Kaplan RM, Wenig LN, Burmeister D. Qualitative ?-hCG urine assays may be misleading in the presence of molar pregnancy: a case report. J Emerg Med 2004;27:43-7.
- Stricklan TW, Puett D. Contribution of subunits to the function of luteinizing hormone/human chorionic gonadotropin recombinants. Endocrinology 1981;109:1933-42.
- Wehmann RE, Blithe DL, Flack MR, Nisula BC. Metabolic clearance rate and urinary clearance of purified beta-core. J Clin Endocrinol Metab 1989;69:510-7.
- Papapetrou PD, Nicopoulou SC. The origin of a human chorionic gonadotropin-subunit-core fragment excreted in the urine of patients with cancer. Acta Endocrinol 1986;112:415-22.
- Cited from http://hubpages.com/hub/Symptomps_of_Cancer.
- Er TK, Jong YJ, Tsai LY, Cheng HJ, Chen BH. Urine pregnancy testing in two women with cancer. Labmedicine 2007;38:280-1.
- Dawood MY, Saxena BB, Landesman R. Human chorionic gonado- tropin and its subunits in hydatifiform mole and choriocarcinoma. Obstet Gynecol 1977;50:172-81.
- Braunstein GD, Vaitukaitis JL, Carbone PP, Ross GT. Ectopic production of human chorionic gonadotropin by neoplasms. Ann Intern Med 1973;78:39-45.
- Levsky ME, Handler JA, Suarez RD, Esrig ET. False-positive urine beta-HCG in a women with a tubo-ovarian abscess. J Emerg Med 2001;2:407-9.
- Kountz DS, Kolander SA, Rozovsky A. False-positive pregnancy test in the Nephrotic syndrome. N Engl J Med 1989;321:1416.