
Monday preference in onset of takotsubo cardiomyopathy
Brief Report
Monday preference in onset of takotsubo cardiomyopathy?
Roberto Manfredini MD?,a, Rodolfo Citro MD b, Mario Previtali MD c, Olga Vriz MD d, Quirino Ciampi MD e, Marco Pascotto MD f, Ercole Tagliamonte MD g,
Gennaro Provenza MD b, Fabio Manfredini MD h, Eduardo Bossone MD, PhD i for the Takotsubo Italian Network investigators
aDepartment of Clinical and Experimental Medicine, Clinica Medica and Vascular Diseases Center, University of Ferrara, 44100 Ferrara, Italy
bCardiology Division, San Luca Hospital, Vallo della Lucania (SA) 84078, Italy cCardiology Division IRCCS San Matteo, University of Pavia, Pavia 27100, Italy dCardiology Division ASS 4, Hospital of San Daniele del Friuli (UD) 33038, Italy eCardiology Division, Fatebenefratelli Hospital, Benevento 82100, Italy fCardiology Division, Fatebenefratelli Hospital, Naples 80100, Italy
gCardiology Division, Hospital Umberto I, Nocera Inferiore (SA) 84014, Italy
hVascular Rehabilitation Program and Vascular Diseases Center, University of Ferrara, 44100 Ferrara, Italy
iInstitute of Clinical Physiology, National Research Council, Lecce 73100, Italy
Received 4 March 2009; revised 30 March 2009; accepted 16 April 2009
Abstract
Objective: Acute cardiovascular events show definite temporal patterns of occurrence. Takotsubo cardiomyopathy (TTC) has been recently shown to exhibit a seasonal (summer) and circadian (morning) temporal distribution. The aim of this study, based on the database of a multicenter Italian network, was to investigate the possible existence of a weekly pattern of onset of TTC.
Methods: The study included all cases of TTC admitted to the coronary care unit of 8 referral cardiac centers in Italy (five in Southern Italy and three in Northern Italy, respectively), belonging to the Takotsubo Italian Network (January 2002-December 2008). Day of admission was categorized into seven 1-day intervals according by week, and chronobiological analysis was performed by partial Fourier series.
Results: The database included 112 patients with TTC (92.9% females). The weekly distribution identified the highest number of cases on Monday and the lowest on Saturday. Chronobiologic analysis yielded a rhythmic pattern with a significant peak on Monday (P = .036).
Conclusions: This study confirms a Monday preference for TTC occurrence on Monday, similar to that reported for acute myocardial infarction. Stress of starting weekly day life activities, could play a triggering role.
(C) 2010
? Funding support: supported, in part, by a scientific grant “Finanziamento per ricerca locale - FAR” from the University of Ferrara, Italy.
* Corresponding author. Tel.: +39 0532 236817; fax: +39 0532 236816.
E-mail addresses: [email protected], [email protected] (R. Manfredini).
0735-6757/$ - see front matter (C) 2010 doi:10.1016/j.ajem.2009.04.023
Introduction
It is known that acute cardiovascular events show definite temporal patterns of onset, for example, circadian, seasonal, and weekly. In fact, cardiac arrests, acute myocardial infarction (AMI) and sudden death, stroke, rupture or dissection of aortic aneurysms, and pulmonary embolism exhibit a circadian (morning) preference [1-7] as well as a seasonal (winter) pattern [8-14].
Takotsubo cardiomyopathy (TTC) is a novel cardiac syndrome, first described in Japan. The definition originates from the Japanese words tako (octopus) and tsubo (jar), since the authors who first named this syndrome observed at the ventriculogram that the heart looked like to the round- bottomed, narrow-necked jar used for trapping the octopus in Japan. This syndrome is of high interest for emergency medicine physicians because it is usually triggered by severe emotional and/or physical stress and generally mimics the clinical scenario of AMI [15]. Some authors have estimated that approximately 2% of ST-elevation acute coronary syndromes referring to their hospital were consistent with TTC [16].
As for temporal pattern of occurrence of cardiovascular acute diseases, both a circadian and seasonal pattern, with respective peaks in the morning hours, and in the summer months, has been recently reported for the onset of TTC in a multicenter series of patients in Italy [17]. On one hand, the morning peak resembles that of AMI [2]. On the other, the seasonal summer pattern of TTC is quite opposite to that of AMI, who is most prominent in winter [8]. Since a Monday preference in the onset of AMI has been described [18], and no information is available for TTC, the aim of this study was to investigate the possible existence of a weekly pattern of onset of TTC as well.
Methods
The analysis included all consecutive patients with TTC admitted between January 2002 and December 2008 to the coronary care unit (CCU) of 8 referral cardiac centers (5 in Southern Italy and 3 in Northern Italy, respectively), belonging to the Takotsubo Italian Network (for complete list of centers and investigators — update 31 December 2008 — see the acknowledgment section). All patients were enrolled according to the Mayo Clinic diagnostic criteria for TTC: (1) transient akinesia/dyskinesia beyond a single major coronary artery vascular distribution; (2) no angiographic evidence of significant coronary artery disease; (3) new electrocardiographic ischemic-like abnormalities (either ST- segment elevation or T-wave inversion); (4) absence of intracranial bleeding, pheochromocytoma, myocarditis, or hypertrophic cardiomyopathy [19]. Clinical variables were recorded in part retrospectively (January 1, 2002-December 31, 2004), and in part prospectively (January 1, 2005-31
December 2008) on a standardized form that included information on patient demographics (sex, age, date and time of onset), signs and symptoms at the event, medical history, trigger events, electrocardiographic ST change at admission, clinical observations during hospitalization (included major cardiovascular complications), T troponin level peak and imaging studies (cardiac catheterization and echocardiography). Retrospective data were recorded by searching hospital discharge diagnosis records and CCU and catheterization laboratory databases. Day of admission was categorized into seven 1-day intervals according by week for analysis, and cases were also analyzed on the basis of their occurrence on weekend versus weekdays. Weekend was defined as any Saturday or Sunday (the period from midnight between Friday and Saturday until midnight between Sunday and Monday). The distribution of admis- sions was tested for uniformity in all groups by the ?2 test goodness of fit [20]. The chronobiological analysis was performed by applying a partial Fourier analysis to the time series data using the validated software Chronolab, written for Macintosh computer [21]. This method selects the harmonic, or the combination of harmonics, that best explain the variance of the time series data. The percentage of the overall variability of the data about the arithmetic mean that is attributable to the fitted rhythmic function (cosine curve by the method of least squares) estimates the goodness of fit of the approximating model, and the F-test statistic is used to test the zero-amplitude null hypothesis (absence of periodi- city). The method calculates the peak and trough time, indicating, respectively, the absolute maximum and mini- mum values during the week. Significance levels were assumed for P b .05.
Results
During the considered period, the Takotsubo Italian Network database included 112 patients with TTC, 104 (92.9%) women, mean age 63.6 +- 10.6 years. Apical form
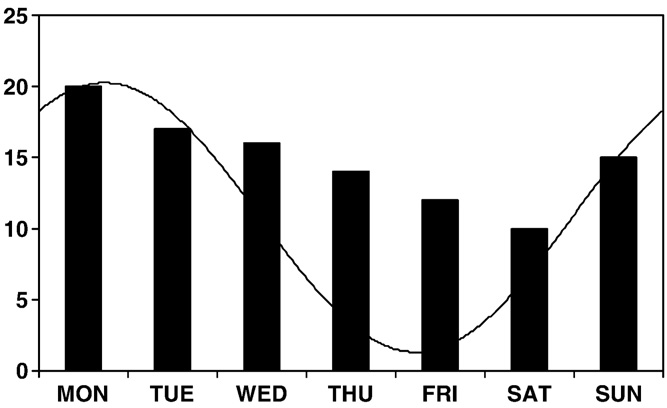
Fig. 1 Weekly distribution of cases of TTC (cosinor fit is superimposed to the graph).
|
Women |
Men |
||
|
Weekdays
|
86 |
79 |
7 |
|
Weekends |
26 |
25 |
1 |
|
Total |
112 |
104 |
8 |
|
?2 |
1.57 |
1.08 |
0.89 |
|
P |
0.211 |
0.299 |
0.347 |
was predominant in 95 patients (84.8%). Trigger events were documented in 74% patients. Presenting symptoms were chest pain in 82 patients (74%), dyspnea in 11 patients (10%), and chest pain associated to dyspnea in 6 patients (5%). Electrocardiogram at hospital admission was char- acterized by ST-segment elevation and non-ST-elevation in 43% and 57% of patients, respectively.
Table 1 Weekdays/weekend distribution of cases of TTC
The weekly distribution (Fig. 1) identified the highest number of cases on Monday and the lowest on Saturday. Inferential chronobiologic analysis yielded a rhythmic pattern in the female group (PR 81%, MESOR 14.86 +- 0.66, amplitude 3.88 +- 0.9, P = .036), characterized by its peak on Monday. Patients admitted on weekdays were 86 (76.8%), and those on weekends were 26 (23.2%). The observed versus expected distribution was not significantly different (Table 1).
Discussion
The main finding of this study was the demonstration of a significant Monday peak in the onset of TTC, in particular, in women. On one hand, it is confirmed that TTC occurs mostly in female population: in our population, the proportion of men was very limited (n = 8, 7.1%), and this did not allow a sufficient statistical power for analysis. On the other, quite similar to the morning pattern of onset, the temporal distribution of TTC resembles that of AMI. Monday, in fact, may be considered a critical day for cardiovascular events. More than a decade ago, Willich et al [22] in Germany, and Gnecchi-Ruscone et al [23] in Italy reported an increased risk of AMI on Monday. In particular, Willich et al. found that this weekly variation with a Monday peak was present only in the working but not in nonworking population. A couple of years after, Spielberg et al [24], in Germany, confirmed the higher frequency of events on Monday, but with no differences between working or retired patients. More recently, Kinjo et al [25] found a Monday peak in working men, but not in women, who exhibited a Saturday peak, and Manfredini et al [26] confirmed this Monday preference also in a large cohort of patients in Italy. Again, a Monday peak was demonstrated also in a series of consecutive patients receiving a third-generation implantable defibrillator [27]. As for sudden death, a Monday peak was reported by Arntz et al [28], in Germany, with an increase more pronounced in patients 65 years or younger than in
patients older than 65 years, and by Gruska et al [29] in Austria, who found that it was irrespective of age and sex, but most pronounced in retired patients, subjects living alone, and persons found unconscious outside buildings or in public places. Finally, a recent meta-analysis study aimed to quantify the excess risk associated with the Monday peak in cardiovascular mortality [30], found an increased pooled odds ratio of 1.19, without significant differences between subgroups by sex and age. Quite similar to AMI, stroke exhibits a Monday preference as well [31], irrespective of sex and the presence or not of the most common risk factors [32]. Among the potential triggering factors, the stress of commencing the weekly working activity has been proposed [33]. Interestingly, stress represents a plausible link to explain the Monday preference of the two similar entities, AMI and TTC. In fact, available evidence is consistent with the concept that extreme emotional and/or physical stress may precede the onset of the clinical presentation of TTC [34]. In these last years, a series of stress-related triggering events have been reported [35-37] (Table 2). The stress-related increased catecholamine level could play a central role in the pathophysiology of TTC by inducing “myocardial stunning” or direct cardiomyocytes injury [38-41], and TTC generally affects women in the postmenopausal period that is characterized by increased sympathetic activity [34]. As for the similarity of the morning peak of AMI and TTC, it is interesting that a morning peak in plasma catecholamines was earlier demonstrated [42] and urinary excretion of norepinephrine was found to be higher during daytime [43]. However, at today, the catecholaminergic hyperactivation is nothing
Table 2 Stress-related triggering events associated with TTC
Psychological stressors
Earthquake Emotional stress
Emotional argument with her husband
Financial losses Marital discord
News of the death of a loved one
Public performance Quarrelling Spousal departure Traffic accidents
Medical stressors
Cocaine use
Diabetic ketoacidosis Exacerbations of chronic disease
Excess alcohol intake Gastrointestinal bleeding Hypoglycemia
Hypotension
Intensive care admission syndrome Intracranial hemorrhage Methicillin-resistant staphylococcal meningitis Myocardial depression during sepsis
Nosebleeds Pneumothorax Polyangiitis Postanesthetic states Postoperative Respiratory failure Severe pain
more than a speculation because there is no evidence of an increased concentration of catecholamines on Monday.
Conclusions
To the best of our knowledge, this is the first report of a significant weekly pattern of TTC events. Emergency medicine physicians are aware that different types of emergency calls exhibit distinct temporal patterns along the day [44]. However, also day-of-week variability might be taken into account, at least for cardiovascular acute events. Additional studies will be needed in order to investigate the potential causes of the Monday preference in the onset of TTC, the possible relationships with stressful events, for example, working activity or only starting weekly day life.
Probably, we could add “Monday” to the long list of stressful factors capable to favor the onset of TTC.
Acknowledgments
Takotsubo Italian Network Principal investigators:
R Citro; Cardiology Division, San Luca Hospital, Vallo della Lucania (SA), Italy
E Bossone; Institute of Clinical Physiology, National Research Council, Lecce, Italy
Coinvestigators:
M.M. Patella, G. Provenza, G. Gregorio; Cardiology Division, San Luca Hospital, Vallo della Lucania (SA), Italy
M. Previtali; Cardiology Division, IRCCS San Matteo, University of Pavia, Italy
O. Vriz; Cardiology Division, ASS 4, Hospital of San Daniele del Friuli (UD), Italy
Q. Ciampi; Cardiology Division, Fatebenefratelli Hospi- tal, Benevento, Italy
C. Astarita; Cardiology Division, Santa Maria Hospital, Sorrento (NA), Italy
M. Pascotto; Cardiology Division, Fatebenefratelli Hos- pital, Napoli, Italy
E. Tagliamonte; Cardiology Division, Hospital Umberto I, Nocera Inferiore (SA), Italy
M. Piepoli, C. Armentano; Cardiology Division, Guglielmo da Saliceto Hospital, Piacenza, Italy
R. Manfredini, F. Manfredini, B. Boari, R. Salmi, M. Gallerani; Vascular Diseases Center, University of Ferrara, Italy
References
- Levine RL, Pepe PE, Fromm RE, et al. Prospective evidence of a circadian rhythm for out-of-hospital cardiac arrests. JAMA 1992;267: 2935-7.
- Muller JE, Stone PH, Turi ZG, et al. Circadian variation in the frequency of onset of acute myocardial infarction. N Engl J Med 1985; 313:1315-22.
- Muller JE, Ludmer PL, Willich SN, et al. Circadian variation in the frequency of onset of sudden cardiac death. Circulation 1987;75: 131-8.
- Marler JR, Price TR, Clark GL, et al. Morning increase in onset of ischemic stroke. Stroke 1989;20:473-6.
- Casetta I, Granieri E, Portaluppi F, Manfredini R. Circadian variability in hemorrhagic stroke. JAMA 2002;287:1266-7.
- Manfredini R, Portaluppi F, Salmi R, et al. Circadian variation in spontaneous rupture of abdominal aorta. Lancet 1999;353:643-4.
- Gallerani M, Manfredini R, Ricci L, et al. Sudden death from pulmonary thromboembolism: chronobiological aspects. Eur Heart J 1992;13:661-5.
- Ornato JP, Peberdy MA, Chandra NC, Bush DE. Seasonal pattern of acute myocardial infarction in the National Registry of Myocardial Infarction. J Am Coll Cardiol 1996;28:1684-8.
- Manfredini R, Boari B, Smolensky MH, et al. Seasonal variation in onset of myocardial infarction-a 7-year single-center study in Italy. Chronobiol Int 2005;22:1097-111.
- Kelly-Hayes M, Wolf PA, Kase CS, et al. Temporal patterns of stroke onset. The Framingham Study. Stroke 1995;26:1343-7.
- Gallerani M, Portaluppi F, Maida G, et al. Circadian and circannual rhythmicity in the occurrence of subarachnoid hemorrhage. Stroke 1996;27:1793-7.
- Manfredini R, Portaluppi F, Salmi R, et al. Seasonal variation in the occurrence of non traumatic rupture of thoracic aorta. Am J Emerg Med 1999;17:672-4.
- Mehta HR, Manfredini R, Hassan F, et al. Chronobiological patterns of acute aortic dissection. Circulation 2002;106:1110-5.
- Gallerani M, Boari B, Smolensky MH, et al. Seasonal variation in occurrence of pulmonary embolism: analysis of the database of the Emilia-Romagna region, Italy. Chronobiol Int 2007;24:143-60.
- Kolkebeck TE, Cotant CL, Krasuski RA. Takotsubo cardiomyopathy: an unusual syndrome mimicking an ST-elevation myocardial infarc- tion. Am J Emerg Med 2007;25:92-5.
- Bybee KA. Clinical characteristics and thrombolysis in myocardial infarction frame counts in women with transient left ventricular apical ballooning syndrome. Am J Cardiol 2004;94:343-6.
- Citro R, Bossone E, Previtali M, et al. Chronobiological patterns of onset of tako-tsubo cardiomyopathy. A multicenter Italian study. J Am Coll Cardiol 2009;54(2):180-1.
- Boari B, Salmi R, Gallerani M, et al. Acute myocardial infarction: circadian, weekly, and seasonal patterns of occurrence. Biol Rhythm Res 2007;38:155-67.
- Bybee KA, Kara T, Prasad A, et al. Systematic review: transient left ventricular apical ballooning: a syndrome that mimics ST- segment elevation myocardial infarction. Ann Intern Med 2004;141: 858-65.
- Snedecor GW, Cochran WG. Statistical methods. Ames (Iowa): Iowa State University Press. 7th ed.; 1980. p. 236-8.
- Mojon A, Fernandez JR, Hermida RC. Chronolab: an interactive software package for chronobiologic time series analysis written for the Macintosh computer. Chronobiol Int 1992;9:403-12.
- Willich SN, Lowel H, Lewis M, et al. Weekly variation of acute myocardial infarction: increased Monday risk in the working population. Circulation 1994;90:87-93.
- Gnecchi-Ruscone T, Piccaluga E, Guzzetti S, et al. Mornings and Monday: critical periods for the onset of acute myocardial infarction. Eur Heart J 1994;15:882-7.
- Spielberg C, Falkenhahm D, Willich SH, et al. Circadian, day of week and seasonal variability in myocardial infarction: comparison between working and retired patients. Am Heart J 1996;132:579-84.
- Kinjo K, Sato H, Sato H, et al. Variation during the week in the incidence of acute myocardial infarction: increased risk for Japanese women on Saturdays. Heart 2003;89:398-403.
- Manfredini R, Manfredini F, Boari B, et al. Seasonal and weekly patterns of hospital admissions for nonfatal and fatal myocardial infarction. Am J Emerg Med [in press].
- Peters RW, McQuillan S, Resnick SK, Gold MR. Increased Monday incidence of life-threatening ventricular arrhythmias. Experience with a third-generation implantable defibrillator. Circulation 1996;94: 1346-9.
- Arntz HR, Willich SN, Schreiber C, et al. Diurnal, weekly, and seasonal variation of sudden death. Population-based analysis of 24,061 consecutive cases. Eur Heart J 2000;21:315-20.
- Gruska M, Gaul GB, Winkler M, et al. Increased occurrence of out-of- hospital cardiac arrest on Mondays in a community-based study. Chronobiol Int 2005;20:401-6.
- Witte DR, Grobbee DE, Bots ML, Hoes AW. Meta-analysis of excess cardiac mortality on Monday. Eur J Epidemiol 2005;20: 401-6.
- Manfredini R, Casetta I, Paolino E, et al. Monday preference in onset of ischemic stroke. Am J Med 2001;111:401-3.
- Manfredini R, Manfredini F, Boari B, Salmi R, Gallerani M. The Monday peak in the onset of ischemic stroke is independent of major risk factors. Am J Emerg Med 2009;27:244-6.
- Murakami S, Otsuka K, Kubo Y, et al. Repeated ambulatory monitoring reveals a Monday morning surge in blood pressure in a community-dwelling population. Am J Hypertens 2004;17(12 Pt 1): 1179-83.
- Sharkey SW, Lesser JR, Zenovich AG, et al. Acute and reversible cardiomyopathy provoked by stress in women from the United States. Circulation 2005;111:472-9.
- Geninatti M, Thames M. All stressed out and no pump to go. Am J Emerg Med 2007;25:202-7.
- Ohigashi-Suzuki S, Saito Y, Tatsuno I. Takotsubo cardiomyopathy associated with sepsis in type 2 diabetes mellitus. Am J Emerg Med 2007;25:230-2.
- Makaryus AN, Patrick C, Patcha R, Maccaro P. Cardiac arrest in a patient with normal coronary arteries. Am J Emerg Med 2008;26:734.e5-7.
- Wittstein IS, Thiemann DR, Lima JA, et al. Neurohumoral features of myocardial stunning due to sudden emotional stress. N Engl J Med 2005;352:539-48.
- Kume T, Akasaka T, Kawamoto T, et al. Assessment of coronary microcirculation in patients with Takotsubo-like left ventricular dysfunction. Circ J 2005;69:934-9.
- Elesber A, Lerman A, Bybee KA, et al. Myocardial perfusion in apical ballooning syndrome correlate of myocardial injury. Am Heart J 2006; 152:469.e9-e13.
- Nef HM, Mollmann H, Kostin S, et al. Tako-tsubo cardiomyopathy: intraindividual structural analysis in the acute phase and after functional recovery. Eur Heart J 2007;352:539-48.
- Turton MB, Deegan T. Circadian variation of plasma catecholamine, cortisol and immunoreactive insulin concentrations in supine subjects. Clin Chim Acta 1974;55:389-97.
- Kurisu S, Inoue I, Kawagoe T, et al. Circadian variation in the occurrence of tako-tsubo cardiomyopathy: comparison with acute myocardial infarction. Int J Cardiol 2007;115:270-1.
- Manfredini R, la Cecilia O, Boari B, et al. Circadian pattern of emergency calls: implications for ED organization. Am J Emerg Med 2002:282-6.