



Flank pain is a common complaint in the emergency department, and the most frequent
cause of flank pain is urolithiasis. Spontaneous renal artery dissection and renal
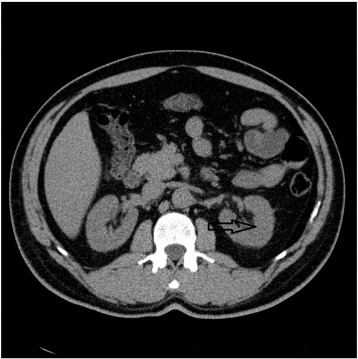
artery thrombosis are rare causes of abdominal pain which can result in renal parenchymal
injury. They are mostly difficult to diagnose and treat in the emergency setting.
The present report describes 2 patients admitted to the emergency department because
of acute flank pain who were diagnosed with renal infarction.
To read this article in full you will need to make a payment
One-time access price info
- For academic or personal research use, select 'Academic and Personal'
- For corporate R&D; use, select 'Corporate R&D; Professionals'
Subscribe:
Subscribe to The American Journal of Emergency MedicineAlready a print subscriber? Claim online access
Already an online subscriber? Sign in
Register: Create an account
Institutional Access: Sign in to ScienceDirect
References
- Pal Isolated Spontaneous Renal Artery Dissection Presented with Flank Pain.Case Rep Radiol. 2015; 2015: 896706
- Spontaneous renal artery dissection.Mo Med. 2010; 107: 124-126
- Spontaneous renal artery dissection: three cases and clinical algorithms.J Hum Hypertens. 2006; 20: 710-718
- Renal infarction caused by spontaneous renal artery dissection: treatment with catheter-directed thrombolysis and stenting.Cardiovasc Intervent Radiol. 2009; 32: 333-336
- Isolated spontaneous renal artery dissection: diagnosis and endovascular management.Diagn Interv Radiol. 2011; 17: 101-104
- Spontaneous recovery from renal infarction resulting from renal artery dissection.Int J Urol. 2005; 12: 405-408
- Contrast induced nephropathy: updated ESUR Contrast Media Safety Committee guidelines.Eur Radiol. 2011; 21: 2527-2541
- Contrast-induced acute kidney injury and renal support for acute kidney injury: a KDIGO summary (part 2).Crit Care. 2013; 17: 205
Article Info
Publication History
Published online: September 09, 2015
Accepted:
September 1,
2015
Received:
August 17,
2015
Identification
Copyright
© 2015 Elsevier Inc. Published by Elsevier Inc. All rights reserved.
