



Abstract
Background
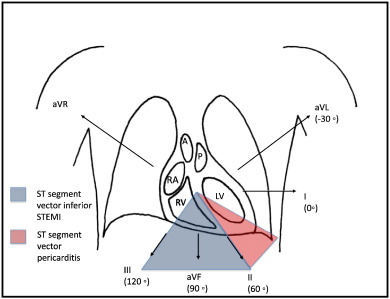
ST-segment elevation (STE) due to inferior STE myocardial infarction (STEMI) may be
misdiagnosed as pericarditis. Conversely, this less life-threatening etiology of ST
elevation may be confused for inferior STEMI.
We sought to determine if the presence of any ST-segment depression in lead aVL would
differentiate inferior STEMI from pericarditis.
Methods
Retrospective study of 3 populations. Cohort 1 included patients coded as inferior
STEMI, cohort 2 included patients with a discharge diagnosis of pericarditis who presented
with chest pain and at least 0.5 mm of ST elevation in at least 1 inferior lead. We
analyzed the presenting electrocardiogram in both populations, with careful assessment
of leads II, III, aVF, and aVL. In addition, we retrospectively studied a third cohort
of patients with subtle inferior STEMI (<1-mm STE with occluded artery on catheterization) and assessed the sensitivity of
ST depression in lead aVL for this group.
Results
Of 154 inferior STEMI patients, 154 had some amount of ST depression in lead aVL (100%;
confidence interval, 98%-100%). Of the 49 electrocardiograms in the pericarditis group,
all 49 had some inferior STE but none had any ST-segment depression in lead aVL (specificity,
100%; confidence interval, 91%-100%). In the third cohort, there were 272 inferior
MIs with coronary occlusion, of which 54 were “subtle.” Of these, 49 had some ST depression
in lead aVL.
Conclusion
When there is inferior ST-segment elevation, the presence of any ST depression in
lead aVL is highly sensitive for coronary occlusion in inferior myocardial infarction
and very specific for differentiating inferior myocardial infarction from pericarditis.
To read this article in full you will need to make a payment
One-time access price info
- For academic or personal research use, select 'Academic and Personal'
- For corporate R&D; use, select 'Corporate R&D; Professionals'
Subscribe:
Subscribe to The American Journal of Emergency MedicineAlready a print subscriber? Claim online access
Already an online subscriber? Sign in
Register: Create an account
Institutional Access: Sign in to ScienceDirect
References
- ST-segment elevation in conditions other than acute myocardial infarction.NEJM. 2003; 349: 2128-2135
- Electrocardiographic ST-segment elevation: the diagnosis of acute myocardial infarction by morphologic analysis of the ST segment.Acad Emerg Med. 2001; 8: 961-967
- Differential characteristics of the electrocardiogram in early repolarizations and acute pericarditis.NEJM. 1976; 295: 523-526
- Usefulness of ST elevation II/III ratio and ST deviation in lead I for identifying the culprit artery in inferior wall MI.Am J Cardiol. 2000; 86: 341-343
- The heart, arteries, and veins.in: 4th ed. McGraw-Hill, New York1978: 1163
- Usefulness of ST segment elevation in lead III exceeding that of lead II for identifying the location of the totally occluded coronary artery in inferior wall MI.Am J Cardiol. 1998; 81: 918-919
- The heart, arteries, and veins.in: 4th ed. McGraw-Hill, New York1978: 1182
- Electrocardiographic differentiation of early repolarization from subtle anterior ST-segment elevation myocardial infarction.Ann Emerg Med. 2012; 60: 45-56
- Incidence, angiographic features, and outcomes of patients presenting with subtle ST-elevation myocardial infarction.Am Heart J. 2014; 168: 884-890
- ST elevation in anterior acute myocardial infarction differs with different methods of measurement.Acad Emerg Med. 2006; 13: 406-412
- T/QRS amplitude ratio best distinguishes the ST elevation of anterior left ventricular aneurysm from anterior acute myocardial infarction.Am J Emerg Med. 2005; 23: 279-287
- ST segment elevation: causes and diagnostic accuracy.J Emerg Med. 1998; 16: 797-798
- Evaluation of ST Segment elevation criteria for the prehospital electrocardiographic diagnosis of acute myocardial infarction.Ann Emerg Med. 1994; 23: 17-24
- ST segment depression in aVL: a sensitive marker for acute inferior myocardial infarction.Eur Heart J. 1992; 14: 4-7
- Acute pericarditis: diagnostic cues and common electrocardiographic manifestations.Cardiol Rev. 2007; 15: 24-30
- The electrocardiogram in acute pericarditis: distributions of morphologic and axial changes in stages.Prog Cardiovasc Dis. 1974; 33: 470-474
- Evaluating a rule for differentiating pericardial disease from ST-segment elevation myocardial infarction.Acad Emerg Med. 2011; 18: s18
Article Info
Publication History
Published online: October 02, 2015
Accepted:
September 30,
2015
Received in revised form:
September 26,
2015
Received:
June 5,
2015
Footnotes
�?�No grants or external funding was used for this manuscript.
�?��?�Abstract presented previously at: ACEP 2013; Denver, CO; October 9, 2013.
Identification
Copyright
© 2015 Elsevier Inc. Published by Elsevier Inc. All rights reserved.
