



Abstract
Objective
Homelessness is a critical public health issue and socioeconomic epidemic associated
with a disproportionate burden of disease and significant decrease in life expectancy.
We compared emergency care utilization between individuals with documented homelessness
to those enrolled in Medicaid without documented homelessness.
Methods
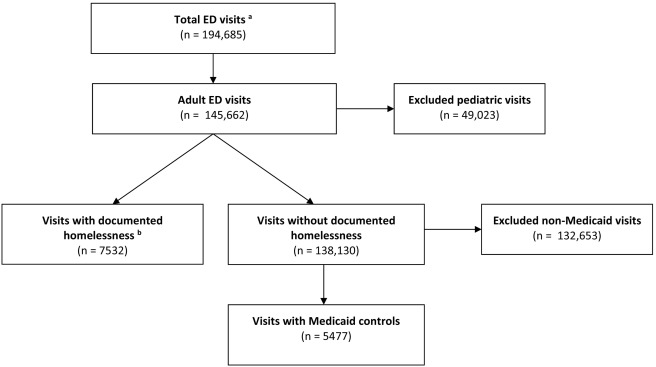
We conducted a retrospective cohort study consisting of electronic medical record
review of demographics, chief complaints, and health care utilization metrics of adults
with homelessness compared to a group enrolled in Medicaid without identified homelessness.
The chart review spanned two years of emergency visits at a single urban, academic,
tertiary care medical center. Descriptive statistics, bivariate and multivariate analyses
were utilized.
Results
Over the study period, 986 patients experiencing homelessness accounted for 7532 ED
visits, with a mean of 7.6 (SD 19.9) and max of 316 visits. The control group of 3482
Medicaid patients had 5477 ED visits, with a mean of 1.6 visits (SD 2.1) and max of
49 visits. When controlling for age, sex, race, ethnicity, and ESI, those living with
homelessness were 7.65 times more likely to return to the ED within 30 days of their
previous visit, 9.97 times more likely to return within 6 months, 10.63 times more
likely to return within one year, and 11 times more likely to return within 2 years.
Conclusions
Compared to non-homeless Medicaid patients, patients with documented homelessness
were over seven times more likely to return to the ED within 30 days and over eleven
times more likely to return to the ED in two years.
Keywords
To read this article in full you will need to make a payment
Subscribe to The American Journal of Emergency Medicine
Already a print subscriber? Claim online access
Already an online subscriber? Sign in
Register: Create an account
Institutional Access: Sign in to ScienceDirect
References
- The 2016 annual homeless assessment report (AHAR) to congress.(Available at)https://www.hudexchange.info/resources/documents/2016-AHAR-Part-1.pdfDate: 2016Date accessed: March 31, 2017
- Comparative cost analysis of housing and case management program for chronically ill homeless adults compared to usual care.Health Serv Res. 2012; 47: 523-543
- Health care utilization patterns of homeless individuals in Boston: preparing for Medicaid expansion under the Affordable Care Act.Am J Public Health. 2013; 103: S311-S317
- Deriving costs of service use among an urban homeless population.J Subst Abus Treat. 2014; 46: 491-497
- Frequent emergency department visits and hospitalizations among homeless people with Medicaid: implications for Medicaid expansion.Am J Public Health. 2015; 105: S716-S722
- Emergency department use among the homeless and marginally housed: results from a community-based study.Am J Public Health. 2002; 92: 778-784
- Health status and health care experiences among homeless patients in federally supported health centers: findings from the 2009 patient survey.Health Serv Res. 2013; 48: 992-1017
- New to care: demands on a health system when homeless veterans are enrolled in a medical home model.Am J Public Health. 2013; 103: S374-S379
- Homeless in America: injuries treated in US emergency departments, 2007–2011.Int J Inj Control Saf Promot. 2014; 21: 289-297
- Characteristics of emergency department visits by older versus younger homeless adults in the United States.Am J Public Health. 2013; 103: 1046-1051
- The homeless orthopaedic trauma patient: follow-up, emergency room usage, and complications.J Orthop Trauma. 2014; 28: e128-e132
- Homelessness as an independent risk factor for mortality: results from a retrospective cohort study.Int J Epidemiol. 2009; 38: 877-883
- Mortality among homeless adults in Boston: shifts in causes of death over a 15-year period.JAMA Intern Med. 2013; 173: 189-195
- Premature mortality in homeless populations: a review of the literature.National Health Care for the Homeless Council, Inc., 2005 (Available at)http://sbdww.org/wp-content/uploads/2011/04/PrematureMortalityFinal.pdfDate accessed: March 31, 2017
- A comprehensive assessment of health care utilization among homeless adults under a system of universal health insurance.Am J Public Health. 2013; 103: S294-S301
- Socio-demographic and clinical characteristics of re-presentation to an Australian inner-city emergency department: implications for service delivery.BMC Public Health. 2007; 7: 320
- The revolving hospital door: hospital readmissions among patients who are homeless.Med Care. 2013; 51: 767-773
- Use of acute care services among older homeless adults.JAMA Intern Med. 2013; 173: 1831-1834
- Predictors of frequent emergency room visits among a homeless population.PLoS One. 2015; 10e0124552
- Predictors of frequent emergency department use among patients with psychiatric illness.Gen Hosp Psychiatry. 2014; 36: 716-720
- Frequent emergency department use by individuals seeking mental healthcare: a systematic search and review.Arch Psychiatr Nurs. 2013; 27: 171-178
- Characteristics of frequent users of the emergency department in the general adult population: a systematic review of international healthcare systems.Health Policy Amst Neth. 2016; 120: 452-461
- Increased 30-day emergency department revisits among homeless patients with mental health conditions.West J Emerg Med. 2016; 17: 607-612
- Food insecurity is associated with greater acute care utilization among HIV-infected homeless and marginally housed individuals in San Francisco.J Gen Intern Med. 2013; 28: 91-98
- Food insufficiency and health services utilization in a national sample of homeless adults.J Gen Intern Med. 2011; 26: 627-634
- Homeless and older veterans may be at risk for malnutrition and food insecurity.Popul Health Manag. 2017; 20: 419
- Effectiveness of interventions to improve the health and housing status of homeless people: a rapid systematic review.BMC Public Health. 2011; 11: 638
- How can health care systems effectively deal with the major health care needs of homeless people?.(Available at)
- Effect of a housing and case management program on emergency department visits and hospitalizations among chronically ill homeless adults: a randomized trial.JAMA. 2009; 301: 1771-1778
- Effectiveness of housing first with intensive case management in an ethnically diverse sample of homeless adults with mental illness: a randomized controlled trial.PLoS One. 2015; 10e0130281
- Permanent patients: hospital discharge planning meets housing insecurity.Hast Cent Rep. 2017; 47: 6-7
- Medical care of the homeless: an American and international issue.Prim Care. 2017; 44: 57-65
- Increasing overall well-being is salient in treating homelessness.Soc Work Public Health. 2017; 32: 154-165
- Factors associated with the health care utilization of homeless persons.JAMA. 2001; 285: 200-206
- Homeless patients' use of urban emergency departments in the United States.J Ambul Care Manag. 2015; 38: 48-58
- Identifying homelessness using health information exchange data.J Am Med Inform Assoc. 2015; 22: 682-687
- Emergency Severity Index (ESI): a triage tool for emergency department care.(Available at)https://www.ahrq.gov/sites/default/files/wysiwyg/professionals/systems/hospital/esi/esihandbk.pdfDate accessed: August 18, 2017
- The urban homeless: super-users of the emergency department.Popul Health Manag. 2014; 17: 366-371
- Application of implementation science for homeless interventions.Am J Public Health. 2013; 103: S183-S184
- ‘Housing first’ for homeless youth with mental illness.Pediatrics. 2016; 138
- One-year outcomes of a randomized controlled trial of housing first with ACT in five Canadian cities.Psychiatr Serv Wash DC. 2015; 66: 463-469
- Fidelity to the housing first model and variation in health service use within permanent supportive housing.Psychiatr Serv Wash DC. 2015; 66: 1283-1289
Article Info
Publication History
Published online: June 02, 2018
Accepted:
June 1,
2018
Received in revised form:
May 31,
2018
Received:
April 13,
2018
Identification
Copyright
© 2018 Elsevier Inc. All rights reserved.
