Corresponding author at: University of Health Sciences, Department of Emergency Medicine, Haseki Research and Training Hospital, Millet Street, 34096 Fatih/Istanbul, Turkey.
We investigated the efficacy and safety of hydroxychloroquine for empirical treatment of outpatients with confirmed COVID-19.
Methods
In this prospective, single-center study, we enrolled ambulatory outpatients with COVID-19 confirmed by a molecular method who received hydroxychloroquine. The patients were divided into low- and moderate-risk groups based on the Tisdale risk score for drug-associated QT prolongation, and the QT interval was corrected for heart rate using the Bazett formula (QTc). The QTc interval was measured by electrocardiography both pretreatment (QTc1) and 4 h after the administration of hydroxychloroquine (QTc2). The difference between the QTc1 and QTc2 intervals was defined as the ΔQTc. The QTc1 and QTc2 intervals and ΔQTc values were compared between the two risk groups.
Results
The median and interquartile range (IQR) age of the patients was 47.0 (36.2–62) years, and there were 78 men and 74 women. The median (IQR) QTc1 interval lengthened from 425.0 (407.2–425.0) to 430.0 (QTc2; 412.0–443.0) milliseconds (ms). However, this was not considered an increased risk of ventricular tachycardia associated with a prolonged QTc interval requiring drug discontinuation, because none of the patients had a ΔQTc of >60 ms or a QTc2 of >500 ms. Moreover, the median (quartiles; minimum-maximum) ΔQTc value was higher in patients in the moderate-risk group than those in the low-risk group (10.0 [−4.0–18.0; −75.0–51.0] vs. 7.0 [−10.5–23.5; −53.0–59.0 ms]) (p = 0.996). Clinical improvement was noted in 91.4% of the patients, the exceptions being 13 patients who presented with non-serious adverse drug reactions or who had severe COVID-19 and were hospitalized. Adverse effects related to hydroxychloroquine were non-serious and occurred in 52.8% (n = 80) of the patients.
Conclusions
Our findings show that hydroxychloroquine is safe for COVID-19 and not associated with a risk of ventricular arrhythmia due to drug-induced QTc interval prolongation. Additionally, hydroxychloroquine was well tolerated, and there were no drug-related non-serious adverse events leading to treatment discontinuation in the majority of patients who were stable and did not require hospitalization.
In December 2019, cases of atypical pneumonia of unknown etiology were reported in Wuhan City, Hubei Province, China. In January 2020, it was determined that the cause of this atypical pneumonia was a new type of coronavirus that had not been previously detected in humans [
Clinical and microbiological effect of a combination of hydroxychloroquine and azithromycin in 80 COVID-19 patients with at least a six-day follow up: a pilot observational study.
Clinical and microbiological effect of a combination of hydroxychloroquine and azithromycin in 80 COVID-19 patients with at least a six-day follow up: a pilot observational study.
]. The worldwide COVID-19 pandemic (caused by severe acquired respiratory syndrome-coronavirus-2 [SARS-CoV-2]) posed a major threat to public health globally [
]. The first case in Turkey was diagnosed on March 11, 2020; at that time, the COVID-19 pandemic had affected about 2 million people worldwide. The Turkish Ministry of Health established an Advisory Board on Coronavirus Research, which compiled national recommendations on the diagnosis, treatment, and control of COVID-19, the first version of which was published in January 2020 under the title 2019-nCoV Guide [
Clinical and microbiological effect of a combination of hydroxychloroquine and azithromycin in 80 COVID-19 patients with at least a six-day follow up: a pilot observational study.
]. The risk is elevated in elderly patients with cardiac comorbidity, in those using other drugs that prolong the QT interval, and in patients with electrolyte disorders [
]. Therefore, in patients who are starting or currently receiving hydroxychloroquine for COVID-19, assessment of the risk of QT prolongation, and electrocardiogram (ECG) and QTc monitoring should be performed before and during treatment [
]. In patients with a Tisdale risk score of ≤6, ECG monitoring is not required if quarantine and isolation are instituted. In patients with a Tisdale risk score of >6, it is recommended not to start hydroxychloroquine if the baseline QTc is <480 ms [
]. The American College of Cardiology recommends measurement of the QTc interval by ECG 2–4 h after the first dose and discontinuing the drug if the baseline QTc increases by 30–60 ms or the QTc increases to >500 ms in patients on hydroxychloroquine for COVID-19 [
We assessed the efficacy and adverse reactions of hydroxychloroquine in ambulatory patients with COVID-19 admitted to the emergency department (ED).
2. Methods
2.1 Study design and setting
This prospective, single-center, observational study was conducted in accordance with the 1989 Declaration of Helsinki and was approved by the Institutional Review Board of Review Board of Haseki Research and Training Hospital in Istanbul, Turkey (no. 108).. The Advisory Board on Coronavirus Research of the Turkish Ministry of Health approved the study. The study enrolled 152 Turkish outpatients with COVID-19 confirmed by real-time polymerase chain reaction (RT-PCR) of nasopharyngeal or oropharyngeal swab specimens obtained in the ED of our tertiary-care hospital from April 25 to May 30, 2020.
2.2 Selection of participants
Adult patients (≥18 years of age) with complaints of fever and/or cough, and shortness of breath, who were admitted to the ED, confirmed by molecular assay to have COVID-19, and identified for ambulatory follow-up and treatment were included.
Guidance developed by the TurkishMinistry of Health that was distributed to all healthcare institutions in Turkey suggested hydroxychloroquine as a therapeutic option for outpatients with COVID-19 who presented with mild respiratory illness (resting oxygen saturation of >93% while breathing ambient air). The suggested hydroxychloroquine regimen was a loading dose of 400 mg twice on day 1, followed by 400 mg daily (200 mg twice daily) for a further 4 days [
]. No other medications, such as antibiotics, corticosteroids or antipyretics, were prescribed to the patients.
In those who received hydroxychloroquine as outpatients, risk assessment (Tisdale risk scoring system) and QT interval measurement were performed before treatment. Twelve‑lead ECGs were performed pretreatment and 4 h posttreatment. The QT interval was measured manually by a senior cardiologist from lead II of the 12‑lead ECGs. The QT interval was measured from the beginning of the earliest onset of the QRS complex to the end of the T wave. During other rhythms, QT and RR intervals were averaged over all complexes on 6 s rhythm strips or 10 s lead II rhythm strips on the 12‑lead ECGs. QT intervals were corrected for heart rate using the Bazett formula (QTc), as per standard clinical practice [
The QTc interval was recorded pretreatment (QTc1) and 4 h after the first administration of hydroxychloroquine (QTc2). Treatment was not started or discontinued if the QTc1 (Bazett formula) was >500 ms. The difference between the pretreatment (QTc1) and posttreatment (QTc2) QTc intervals (QTc2–QTc1) was defined as the delta QTc (ΔQTc). QTc interval prolongation was defined as a QTc1 of >480 ms, a QTc2 interval of ≥500 ms, or an increase in the QTc interval (ΔQTc) of ≥60 ms compared with the pretreatment value.
Patients with Tisdale risk scores of ≤6 and 7–10 were classified into the low- and medium-risk groups, respectively. The QTc1 and QTc2 intervals were compared between the two groups. The Tisdale risk scoring system is shown in Table 1.
Table 1Tisdale risk score for drug-associated QTc prolongation.
Adverse events including malignant arrhythmia, ventricular tachycardia, nausea, vomiting, diarrhea, dyspepsia, bloating, abdominal pain, headache, and dizziness during hydroxychloroquine treatment were obtained from the electronic medical records. In addition, patients who were readmitted and hospitalized for treatment due to adverse effects, or because symptoms did not regress, or worsened after outpatient discharge, were recorded. After discharge, patients were followed up according to the” stay at home” guidance for households and self-isolated for at least 14 days after their first positive SARS-CoV-2 RT-PCR test [
]. The investigators directly communicated with patients or their families, via “daily wellness” phone calls, to obtain data on adverse side effects during the 2 weeks, and on readmission to the ED.
Patients were excluded if they had a known allergy to hydroxychloroquine or chloroquine, a known contraindication to treatment with the study drug (retinopathy, history of long QT syndrome, and QTc interval prolongation), or had a Tisdale risk score of ≥11. Patients with respiratory distress, SpO2 < 93% at admission, severe pneumonia findings on chest x-ray or chest computed tomography, or poor prognostic criteria (blood lymphocyte count <800/μL, CRP > 40 mg/L, ferritin >500 ng/mL, or D-dimer >1000 ng/mL) in blood tests at the time of admission to the ED were not excluded. Breastfeeding and pregnant patients were excluded based on their declaration and pregnancy test results when required. Patients were informed of the study protocol, and written informed consent was obtained prior to participation in the study.
2.3 Statistical analyses
Data were analyzed using SPSS 24.0 for Windows (IBM, Armonk, NY) and MedCalc (MedCalc, Ostend, Belgium; version 12.1.4). Categorical variables are expressed as numbers and percentages. Quantitative variables are expressed as medians and interquartile range (IQR). The Shapiro–Wilk test was employed to verify the normality of the distributions of quantitative variables. Categorical variables in two independent groups (Tisdale low- vs. moderate-risk groups) were compared by Pearson chi-squared test when the data were normally distributed. The Mann–Whitney U test was used to compare non-normally distributed data (e.g., QTc1 and QTc2 intervals and ΔQTc). The Wilcoxon paired test was used to assess the significance of differences between the pretreatment QTc (QTc1) and posttreatment QTc (QTc2) intervals. The significance level was set at p < 0.05.
3. Results
The study population consisted of 78 male (51.3%) and 74 female (48.7%) patients with confirmed COVID-19 who received ambulatory hydroxychloroquine treatment. Their median age was 47.0 (IQR 36.2–62) years (Table 1). The median (IQR) Tisdale risk score of the patients was 4.0 (3.0–5.0); 87.5% (n = 133) of the patients had a risk score of ≤6 (low risk) and 12.5% (n = 19) had a risk score of 7 to 10 (moderate risk). There was a significant difference between the patients in the low- and moderate-risk groups in age (p < 0.001) but not in sex (p = 0.066).
The most common symptoms on admission were cough in 61.8% (n = 94) of the patients, fever in 51.3% (n = 78), and lassitude and fatigue in 43.4% (n = 66). Of the patients, 53.4% (n = 81) had comorbidities; these were hypertension (21.1%, n = 32), diabetes mellitus (15.1%, n = 23), cardiovascular disease including coronary artery disease (8.6%, n = 13) and chronic heart failure (2%, n = 3), and chronic respiratory diseases such as asthma and chronic obstructive pulmonary disease (6.6%, n = 10). There was a significant difference in the rates of comorbidities between the low- and moderate-risk groups (all p < 0.001; Table 2).
Table 2Demographic and clinical characteristics of the low- and moderate-risk groups.
Characteristic
Low risk score (n = 133)
Tisdale risk scores of ≤6 and 7–10 denote low and medium risks of drug-associated QTc prolongation.
Moderate risk score (n = 19)
Tisdale risk scores of ≤6 and 7–10 denote low and medium risks of drug-associated QTc prolongation.
After hydroxychloroquine treatment, the QTc interval (QTc2) at 4 h was prolonged in 64.5% (n = 98) and shortened in 35.5% (n = 54) of the patients compared to that at admission. There was no significant difference between the low- and moderate-risk groups in terms of QTc2 prolongation or shortening (p = 0.501; Table 2). Also, 14.5% (n = 22) of the patients had a ΔQTc of ≥30 ms, but none had a ΔQTc of ≥60 ms. There was no significant difference between the low- and moderate-risk groups in a ΔQTc of ≥30 ms (p = 0.601; Table 2). The demographic and clinical characteristics of the patients according to Tisdale risk score are listed in Table 2.
The median (IQR) QTc1 interval before hydroxychloroquine treatment was 425.0 (407.2–425.0) ms. The median (IQR) QTc2 interval was 430.0 (412.0–443.0) ms at 4 h posttreatment. The median (IQR) ΔQTc was 7.0 ms (−8.7–22.0; −75.0–59.0) (p = 0.001).
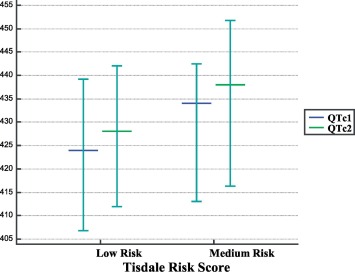
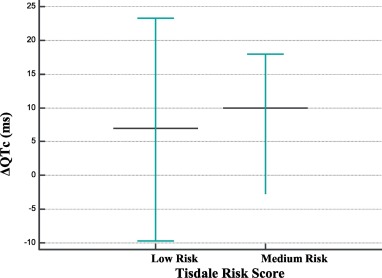
Based on the Tisdale risk score, a median (IQR) QTc1 interval of 424.0 ms (406.5–439.5), a median (IQR) QTc2 of 428.0 ms (412.0–442.0), and a median (quartiles; min-max) ΔQTc of 7.0 (−10.5–23.5; −53.0–59.0) ms were found in the low-risk group (p = 0.002; Table 3 and Fig. 1, Fig. 2). In the moderate-risk group, the median (IQR) QTc1 interval was 434.0 ms (412.0–443.0), the median (IQR) QTc2 was 438.0 ms (416.0–453.0), and the median (quartiles; minimum-maximum) ΔQTc was 10.0 (−4.0–18.0; −75.0–51.0) ms (p = 0.260; Table 3 and Fig. 1, Fig. 2).
Table 3QTc1, QTc2, and ΔQTc interval values in patients in the low- and moderate-risk groups.
Intergroup comparisons (low vs. moderate risk) were conducted by chi-squared and Mann–Whitney U tests, as appropriate.
Characteristic
Low risk score (n = 133)
Moderate risk score (n = 19)
p
QTc1, ms
424.0 (406.5–439.5)
434.0 (412.0–443.0)
0.203
QTc2, ms
428.0 (412.0–442.0)
438.0 (416.0–453.0)
0.246
ΔQTc, ms
7.0 (−10.5–23.5)
10.0 (−4.0–18.0)
0.996
Data are medians and interquartile ranges (IQR).
ΔQTc denotes difference in the pretreatment (QTc1) and posttreatment (QTc2) QTc intervals (QTc2–QTc1).
Intergroup comparisons (low vs. moderate risk) were conducted by chi-squared and Mann–Whitney U tests, as appropriate.
No adverse events related to hydroxychloroquine treatment were recorded in 52.8% (n = 80) of the patients. In contrast, gastrointestinal symptoms in 22.3% (n = 34) (e.g., diarrhea, non-specific abdominal pain, dyspepsia, bloating, nausea, vomiting), headache and dizziness in 16.4% (n = 25), itching and redness in 2.6% (n = 4), metallic mouth, and dry mouth, were detected as non-serious adverse reactions. None of the patients developed anaphylaxis or cardiotoxicity-related malignant cardiac arrhythmia as a serious adverse reaction.
Of the patients, 8.6% (n = 13) were readmitted to the ED with non-serious adverse drug reactions (n = 5) or worsened symptoms (n = 8). Hydroxychloroquine was discontinued and favipiravir (1600 mg twice daily followed by 600 mg twice daily for 5 days), an emerging antiviral option, was started among those with non-serious adverse drug reactions and mild COVID-19; a trend toward clinical improvement was observed over the follow-up. Patients whose symptoms worsened, particularly those with difficulty breathing, were hospitalized and treated with hydroxychloroquine plus azithromycin, the antiviral drug favipiravir, anticoagulation, corticosteroids and supplemental high-flow oxygen, and were also placed in the prone position. At the 7–10-day follow-up in inpatient isolation wards, all patients eventually recovered and were discharged from the hospital.
Also, 91.4% (n = 139) of the patients completed hydroxychloroquine treatment and their symptoms had significantly improved at the 2-week follow-up. By the end of the follow-up period, only 19 patients had unresolved symptoms, including fatigue and lassitude, with the remaining patients reporting progressive resolution of symptoms including fever, cough and shortness of breath.
4. Discussion
The risk of ventricular arrhythmia due to excessive QT prolongation induced by hydroxychloroquine in patients with COVID-19 is unclear. This is the first clinical observational study of the safety and efficacy of hydroxychloroquine for the treatment of outpatients with confirmed COVID-19.
The key findings are as follows: 1) Among 152 patients with confirmed COVID-19, clinical improvement occurred in 91.4%, the exceptions being 13 patients who presented with adverse drug reactions or who progressed to severe infection and were hospitalized. 2) Adverse effects related to hydroxychloroquine were non-serious and occurred in 52.8% (n = 80) of patients; hydroxychloroquine was well tolerated by the other patients. 3) Gastrointestinal symptoms including diarrhea, dyspepsia, nausea, and vomiting were the most common adverse effects of hydroxychloroquine. Additionally, none of the patients experienced anaphylaxis or cardiotoxicity-related malignant cardiac arrhythmia as a serious adverse reaction to hydroxychloroquine. 4) There was no prolongation of QTc2 (to >500 ms or an increase of ≥60 ms) among the patients with COVID-19. The median (IQR) QTc1 interval lengthened from 425.0 (407.2–425.0) ms to 430.0 (412.0–443.0) ms 2–4 h after the first dose of hydroxychloroquine. Also, 14.5% (n = 22) of the patients had a ΔQTc of ≥30 ms and none had a ΔQTc of ≥60 ms. Moreover, the frequency of a ΔQTc interval of >30 ms did not differ between the low- and moderate-risk groups.
Chloroquine and hydroxychloroquine are antimalarial and anti-rheumatic drugs that have been prescribed to billions of people [
]. Although hydroxychloroquine is on the WHO list of essential medicines and is generally well tolerated by patients with no underlying illness, it has several side effects, some of which, particularly cardiac adverse effects, can be fatal [
]. Although chloroquine and hydroxychloroquine have a good safety profile, the American Heart Association considers them to have direct myocardial toxicity and to exacerbate underlying myocardial dysfunction [
Recently, the Food and Drug Administration (FDA) issued emergency authorization for the use of hydroxychloroquine for COVID-19. The FDA had received several reports of safety issues related to hydroxychloroquine in patients with COVID-19, including serious cardiac adverse events and deaths [
]. One of the most serious side effects of hydroxychloroquine for COVID-19 is heart rhythm problems, including excessive QTc prolongation and an elevated risk of torsade de pointes associated with ventricular tachycardia [
]. Patients receiving azithromycin and/or hydroxychloroquine for COVID-19 should be evaluated for the risk of QT prolongation before and during treatment, and their QT interval should be monitored by ECG [
]. This is facilitated by hospitalizing high-risk patients in continuing care units with ECG monitoring or performing ECG in ambulatory patients before and at the beginning of treatment to enable early detection and treatment of any cardiac side-effects [
Urgent guidance for navigating and circumventing the QTc-prolonging and Torsadogenic potential of possible pharmacotherapies for coronavirus disease 19 (COVID-19).
The hydroxychloroquine dose recommended for the treatment of mild, moderate, and severe COVID-19 is 500 mg twice daily for 10 days; therefore, the risk of QT prolongation is likely to be elevated [
Clinical and microbiological effect of a combination of hydroxychloroquine and azithromycin in 80 COVID-19 patients with at least a six-day follow up: a pilot observational study.
]. The dosage used in this pilot study was slightly lower (a loading dose of 400 mg twice on day 1, followed by 400 mg daily for a further 4 days) than that proposed for outpatients with COVID-19. Although previous clinical studies have reported that hydroxychloroquine, which has antiviral effects in vitro, is associated with clinical recovery in patients with COVID-19, the findings of clinical reports assessing the effectiveness of hydroxychloroquine remain controversial [
Clinical and microbiological effect of a combination of hydroxychloroquine and azithromycin in 80 COVID-19 patients with at least a six-day follow up: a pilot observational study.
]. A meta-analysis of 7 randomized controlled trials and 14 cohort studies demonstrated a lack of efficacy of hydroxychloroquine in reducing hospitalizations or short-term mortality in patients with COVID-19 [
An open-label, multicenter, randomized, controlled trial of 667 hospitalized patients with suspected or confirmed mild-to-moderate COVID-19 found no significant difference in the 15-day clinical outcome among groups that received standard care (control group), hydroxychloroquine alone, or hydroxychloroquine plus azithromycin. In the trial, enrolled patients were receiving no more than 4 L/min of supplemental oxygen [
]. A recent study of patients with documented SARS-CoV-2 hypoxemic pneumonia, within 48 h of admission to hospital, compared adding hydroxychloroquine at a dose of 600 mg/day (treatment group) versus standard care without hydroxychloroquine (control group). The results suggested that hydroxychloroquine treatment as an adjunct to standard care was not associated with a reduction of admissions to the intensive care unit or death 21 days after hospital admission compared with standard care alone [
Clinical efficacy of hydroxychloroquine in patients with covid-19 pneumonia who require oxygen: observational comparative study using routine care data.
]. The results of this trial did not support the use of hydroxychloroquine in patients admitted to hospital with COVID-19 who required oxygen but not intensive care. Our pilot study enrolled patients with mild-to-moderate COVID-19 who did not require supplemental oxygen. Thus, hydroxychloroquine might help to prevent disease progression when started earlier in outpatients with confirmed mild COVID-19 who are stable and do not require supplemental oxygen. However, because we included only hemodynamically stable confirmed COVID-19 patients admitted to hospital, we cannot draw any conclusions regarding the efficacy of hydroxychloroquine to prevent severe forms of the disease.
Hydroxychloroquine (or chloroquine) has demonstrated efficacy in Chinese patients with COVID-19 in clinical trials by reducing fever, improving chest computed tomography (CT) findings, and delaying disease progression [
] conducted in 31 Chinese COVID-19 patients treated with 400 mg of hydroxychloroquine per day over 5 days showed significantly shortened body temperature recovery time and cough remission time, and a higher rate of improved pneumonia as assessed by chest CT. In the study by Gautret et al. [
Clinical and microbiological effect of a combination of hydroxychloroquine and azithromycin in 80 COVID-19 patients with at least a six-day follow up: a pilot observational study.
] in a French tertiary-care center involving 80 hospitalized patients with COVID-19 treated with 200 mg of oral hydroxychloroquine sulfate, three times daily for 10 days combined with azithromycin, all patients improved clinically except one 86-year-old patient who died and one 74-year-old patient who remained in intensive care. Finally, another French study involving 36 patients with COVID-19 showed that 600 mg of hydroxychloroquine daily was significantly associated with viral load reduction/disappearance and the effect was augmented by azithromycin [
]. Similarly, in this clinical trial involving 152 patients with COVID-19, the majority of patients treated with hydroxychloroquine (400 mg per day, n = 139 patients) showed significant clinical improvement, and 52.8% exhibited non-serious drug-related side effects (n = 80). Only 8.6% of the patients were hospitalized for adverse drug reactions (n = 5) or worsened symptoms (n = 8).
Although chloroquine and hydroxychloroquine are proarrhythmic and have a risk of ventricular arrhythmia caused by QT prolongation, they are effective for suppressing atrial and ventricular arrhythmias [
]. The most recent guidance from the Mayo Clinic and the American College of Cardiology indicates that in patients with a baseline QTc of <480 ms, the QTc interval should be measured 4 h after the first administration of hydroxychloroquine. Prompt dose reduction or drug discontinuation should be considered if the ΔQTc is >60 ms or the QTc increases to >500 ms after hydroxychloroquine treatment to reduce the risk of malignant arrhythmia [
Urgent guidance for navigating and circumventing the QTc-prolonging and Torsadogenic potential of possible pharmacotherapies for coronavirus disease 19 (COVID-19).
The cardiac safety of chloroquine phosphate treatment in patients with systemic lupus erythematosus: the influence on arrhythmia, heart rate variability and repolarization parameters.
], the influence of 7 months of 250 mg of chloroquine daily on arrhythmia and heart conduction disturbances was evaluated in 28 patients with systemic lupus erythematosus—the QTc interval lengthened from 363 to 388 to 372–392 ms. All of the subjects presented with a sinus rhythm both at enrollment and after treatment. In addition, no episode of paroxysmal arrhythmia or conduction disturbance was reported during the study.
Similarly, none of the patients in this study exhibited malignant arrhythmia due to excessive QT prolongation. Moreover, the median (quartiles; minimum-maximum) ΔQTc value was nonsignificantly higher in the moderate-risk group than in the low-risk group (10.0 [−4.0–18.0; −75.0–51.0] vs. 7.0 [−10.5–23.5; −53.0–59.0 ms]) (p = 0.996). However, this was not considered to require drug discontinuation, because none of the patients had a ΔQTc of >60 ms or a QTc2 of >500 ms. Unlike the few anecdotal reports of cardiac side-effects of hydroxychloroquine due to excessive QT prolongation [
], we determined the cardiac safety profile of hydroxychloroquine at a loading dose of 400 mg twice on day 1 followed by 400 mg daily for a further 4 days in patients with COVID-19.
This study had several limitations. First, it was limited by the single-center small-scale design, limited long-term outcome, and inclusion of only 152 patients with mild COVID-19. Second, a proper control group was lacking, which would be required to demonstrate the efficacy of hydroxychloroquine treatment. Thus, a larger study involving ambulatory patients treated with hydroxychloroquine and including a control group is needed to overcome these issues. Third, we did not perform repeat SARS-Cov-2 PCR to confirm virus clearance, so cannot draw any conclusions about the efficacy of hydroxychloroquine for reducing viral shedding. In addition, in patients with a baseline QTc of <500 ms, a single QTc interval measurement by ECG was performed 4 h after the first administration of hydroxychloroquine, and we were unable to measure the QTc interval after the second to fourth doses, as in a recent report [
]. To limit the risk of exposure to SARS-CoV-2 or infection transmission, a mobile or wireless device should be used for this purpose in future studies.
In conclusion, hydroxychloroquine has a good cardiac safety profile, and so may be used safely for early treatment of patients with mild COVID-19 who are stable and do not require hospitalization. In addition, the prolongation of the QTc interval was greater in the moderate- than the low-risk group. However, the alteration in the QTc interval did not exhibit excessive QT prolongation and did not require drug discontinuation because of an increased risk of cardiac arrhythmia associated with QTc interval prolongation, in both risk groups.
Funding and support
This study was supported by the Advisory Board on Coronavirus Research of the Turkish Ministry of Health.
Author contributions
OÖ.S, MM.C and R.G designed this study. Ö.S, O.K, H.E, TB.Ü, O.D, M.K, T.A, and S.C supervised the overall data collection process, had full access to all the data in the study, and takes responsibility for the integrity of the data. R.G and O.S conducted the data analysis. Öo, R.G and MM.C wrote the initial draft of the article. All authors provided substantial review and feedback on the final version of the article. Ö.S takes responsibility for the paper as a whole.
Declaration of Competing Interest
None.
References
Huang C.
Wang Y.
Li X.
et al.
Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China.
Clinical and microbiological effect of a combination of hydroxychloroquine and azithromycin in 80 COVID-19 patients with at least a six-day follow up: a pilot observational study.
Urgent guidance for navigating and circumventing the QTc-prolonging and Torsadogenic potential of possible pharmacotherapies for coronavirus disease 19 (COVID-19).
Clinical efficacy of hydroxychloroquine in patients with covid-19 pneumonia who require oxygen: observational comparative study using routine care data.
The cardiac safety of chloroquine phosphate treatment in patients with systemic lupus erythematosus: the influence on arrhythmia, heart rate variability and repolarization parameters.




 Intergroup comparisons (low vs. moderate risk) were conducted by chi-squared and Mann–Whitney U tests, as appropriate.
Intergroup comparisons (low vs. moderate risk) were conducted by chi-squared and Mann–Whitney U tests, as appropriate.