



Abstract
The evidence supporting many beliefs in medicine is based upon opinion, personal experience,
hearsay, or "common knowledge." When one searches for the data supporting oft-quoted
facts in medicine, they are sometimes found to be old, incorrect, or nonexistent.
Such unsupported facts or beliefs can be termed myths. This minireview will summarize 4 examples of "myth busting" by the author when he
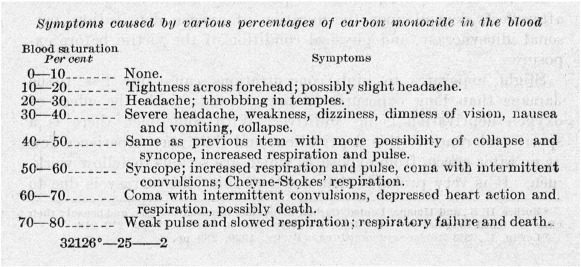
has discovered widely held beliefs regarding carbon monoxide (CO) poisoning to be
untrue during a 25-year career of research in the field. These include the mistaken
beliefs that (1) symptoms correlate with presenting blood carboxyhemoglobin levels,
(2) residents are safe from CO poisoning if their home does not contain fuel-burning
appliances, (3) carboxyhemoglobin levels must be measured rapidly and on arterial
blood, and (4) CO poisoning predisposes to premature long-term death from cardiac
disease. In addition to providing the evidence disproving these myths, the importance
of going back to the original reference when citing prior work is emphasized.
To read this article in full you will need to make a payment
One-time access price info
- For academic or personal research use, select 'Academic and Personal'
- For corporate R&D; use, select 'Corporate R&D; Professionals'
Subscribe:
Subscribe to The American Journal of Emergency MedicineAlready a print subscriber? Claim online access
Already an online subscriber? Sign in
Register: Create an account
Institutional Access: Sign in to ScienceDirect
References
- Environmental emergencies: carbon monoxide poisoning.in: Howard P.K. Steinromm R.A. Sheehy’s emergency nursing: principles and practice. 6th ed. Moseby/Elsevier, St. Louis2010: 544-545
- Carbon monoxide.in: Wolfson A.B. Clinical practice of emergency medicine. 4th ed. Lippincott, Williams, and Wilkins, Philadelphia1998: 1579
- Carbon monoxide poisoning: a review for clinicians.J Emerg Med. 1999; 17: 87-93
- MRI and neuropsychological correlates of carbon monoxide exposure: a case report.Environ Health Perspect. 2002; 110: 1051-1055
- Technology demonstration of a prototype low carbon monoxide electrical generator.([Accessed October 15, 2015])
- Symptoms of acute carbon monoxide poisoning do not correlate with the initial carboxyhemoglobin level.Undersea Hyperb Med. 2012; 2: 657-665
- Carbon monoxide exposure and carboxyhemoglobin.Environ Health Perspect. 2003; 111: A511-A512
- Dangers of and treatment for carbon monoxide poisoning.Bureau of Mines reports of investigations, 1923 ([serial number 2476, 11 pages])
- Physiological effects of exposure to low levels of carbon monoxide.Public Health Rep. 1922; 37: 1127-1142
- Partnering with a medical society to perform online disease surveillance.Undersea Hyperb Med. 2012; 39: 647-655
- Home safety: fire safety laws and legislation.([Accessed September 3, 2015])
- Diffusion of carbon monoxide through gypsum drywall.JAMA. 2013; 310: 745-746
- Relationship between venous and arterial carboxyhemoglobin levels in patients with suspected carbon monoxide poisoning.Ann Emerg Med. 1995; 25: 481-483
- Relationship between arterial, mixed venous, and internal jugular carboxyhemoglobin concentrations at low, medium, and high concentrations in a piglet model of carbon monoxide toxicity.Crit Care Med. 2000; 28: 1998-2001
- Stability of carboxyhemoglobin in stored and mailed blood samples.Am J Emerg Med. 2008; 26: 191-195
- Myocardial injury and long-term mortality in moderate to severe carbon monoxide poisoning.JAMA. 2006; 295: 398-402
- Increased long-term mortality among survivors of acute carbon monoxide poisoning.Crit Care Med. 2009; 37: 1941-1947
Article Info
Publication History
Published online: November 03, 2015
Accepted:
October 30,
2015
Received in revised form:
October 26,
2015
Received:
September 19,
2015
Identification
Copyright
© 2015 Elsevier Inc. Published by Elsevier Inc. All rights reserved.
